
Wednesday, March 22, 2017
0815 – 1545 (EDT)
Lord Elgin Hotel, Lady Elgin Room (lobby level),
100 Elgin Street, Ottawa, Ontario, K1P 5K8
In Attendance
- Sapper (Retired) Aaron Bedard
- Michael Blais, Canadian Veterans Advocacy
- Dr. Karen Cohen, Canadian Psychological Association
- Dave Gallson, Mood Disorders Society of Canada
- Sergeant Brian Harding
- Glynne Hines, Royal Canadian Legion (Co-chair)
- Ed Mantler, Mental Health Commission of Canada (on behalf of Louise Bradley)
- Warrant Officer (Retired) Brian McKenna
- Colonel Scott McLeod, Deputy Surgeon-General, Canadian Armed Forces
- Dr. Patrick Smith, Canadian Mental Health Association
- Robert Thibeau, Aboriginal Veterans Autochtones
Regrets
- Dr. Ruth Lanius, Western University
- Dr. Don Richardson, Canadian Psychiatric Association
Observer
- Commodore (Retired) Andrea Siew, Office of the Veterans Ombudsman (OVO)
Minister’s Office
- Ben Charland, Stakeholder Relations
Veterans Affairs Canada
- Joel Fillion, Director, Mental Health and VAC Mental Health Advisory Group co-chair
- Dr. Jim Thompson, Research Medical Advisor
- Dr. Alexandra Heber, Chief of Psychiatry
- Dr. Sophie Brière, Psychology Consultant
- Katherine Spencer-Ross, Director, Stakeholder Engagement and Outreach
- Marie-Eve Chagnon, Analyst, Stakeholder Engagement and Outreach
Guests
- Colonel Andrew Downes, Director Mental Health, Heath Services Group Headquarters, Canadian Armed Forces
- Lieutenant Colonel, Dave Cameron, Canadian Armed Forces
- Paul Hale, Princess Patricia Canadian Light Infantry (PPCLI) Association
Warning: Please note, some individuals may be disturbed by the content in this document which focuses on suicide. Reading this summary may trigger some discomfort or strong reactions.
The Veterans Affairs Canada (VAC) Mental Health Advisory Group meeting of March 22, 2017 focused mainly on the topic of Veteran suicide.
Presentation: Suicide Prevention for Canadian Armed Forces (CAF) Veterans
Three departmental health professionals presented on suicide prevention efforts from the VAC perspective. The purpose of the presentation was to consult and gather input from the Mental Health Advisory Group on the VAC/CAF Suicide Prevention Strategy and associated Action Plan.
The VAC framework (below) was developed and implemented by VAC in 2010. It captures the multiple factors associated with suicide at different stages of the suicide pathway and helps identify evidence-based interventions to prevent suicide.
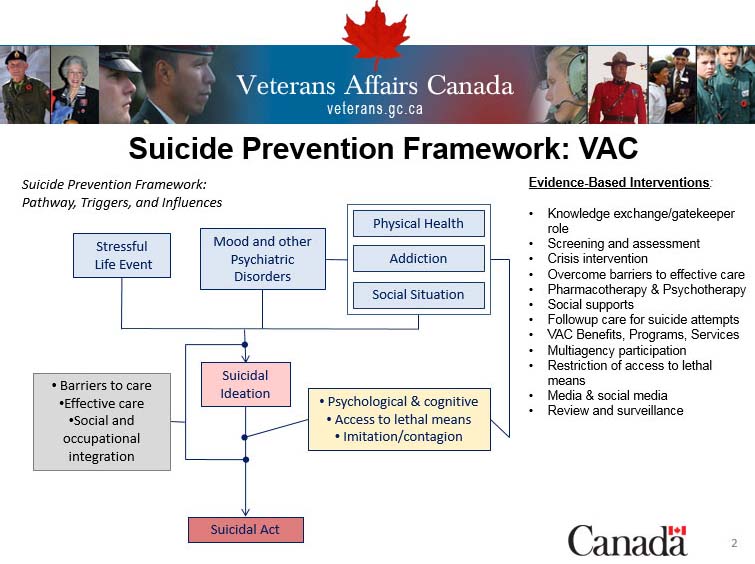
Based on the Mann Model Framework (2005), Mann et al. Suicide prevention strategies: a systematic review. JAMA.2005 Oct 26, 294(16):2064-74.
Since 2010, VAC has taken suicide prevention actions including, but not limited to, reviewing protocols, improving the VAC Assistance Service line, adding suicide indicator “flags” in the administrative database, and conducting case management file reviews (not medical records). For VAC and the CAF, suicide prevention is part of an overall mental health strategy and action plan, which starts at CAF basic training, continues through the transition from CAF to VAC, and carries-on post-release. The VAC/CAF joint suicide prevention strategy has as its mission the prevention of suicide among CAF members and Veterans, using a framework that seeks to understand and address factors that influence suicide across the life course of military members and Veterans. Suicide prevention actions are threefold:
- prevention: preventing suicidal behavior
- intervention: actions when a Veteran becomes suicidal
- postvention: actions after a Veteran has died by suicide.
The discussion was broader than the strategy itself and the following topics were raised:
Suicidality
Presenters reminded the group that suicidality (which encompasses suicidal thinking, suicide attempts and death by suicide) should be considered a multidimensional issue influenced by a multitude of factors: biological, psychological, interpersonal, socio-economic, cultural, spiritual, etc. All influencing factors must be considered in preventing, treating and understanding suicide. VAC medical personnel pointed out that suicidality is a temporary state which can be treated with appropriate intervention.
Members observed that:
- treatment success relates to treating the underlying mental health problem, and disrupting the suicide pathway in other ways, like breaking away from the thoughts of inevitability and hopelessness one can feel
- service members are often resistant to seek help for fear of negative career impact
- having access to Veteran suicide statistics and data would support suicide prevention.
Transition
Members observed that:
- a Veteran’s identity is intricately tied to his or her service; those in transition to post-military life may experience stressors from having to find new sources of well-being, civilian employment, and handling financial uncertainty
- the loss of identity can, when added to other factors and stressors, contribute to a vulnerable state
- the shift from the military’s highly organized, hierarchical structure, to reintegration in civilian life is a challenge
- seamless transition is a priority and should be integrated into the suicide prevention strategy.
Contagion
VAC noted that suicide contagion, which is when a peer’s suicide triggers suicidal behavior in others:
- can occur when individuals have a strong sense of shared identity and a solid bond with their peers
- is observed in student, military, aboriginal and isolated communities
- is why postvention should focus on people within the deceased’s circle and his or her community so that the potential pathway is disrupted
- can occur when media, social media, and even peers, inadvertently glorify suicide, or present dying by suicide as a reasonable option, or disparage mental health treatment, thereby discouraging those who are suffering from seeking help. Media reporting guidelines were presented as a reasonable guide for how to communicate about suicide on social platforms, without contributing to suicide contagion. (Honour the service or the individual, not the manner of death).
Lethal Means
VAC raised the issue of vulnerable people having access to lethal means, and explained that from a professional perspective the intent is to remove access to firearms and other lethal means when a person feels suicidal, because of the increased risks of impulsivity in a moment of despair. The group offered a different perspective:
- for many service members or Veterans who own firearms, the risk of having their weapons removed is actually a deterrent for them to seek help
- peers or family members should step-in and offer to safe-keep firearms until the individual is better. This was reinforced as a good strategy.
Training & Resources
The CAF noted that the Road to Mental Readiness program (R2MR) has been increasing mental health literacy and is working to expand the program’s reach, as well as to reduce stigma associated with mental health issues.
Members mentioned that the CAF leadership can:
- eliminate stigma with better training and education at all levels of leadership
- put the emphasis on testing skills and knowledge instead of expecting the training to be sufficient. A member said “you get what you inspect, not what you expect” and this deeply resonated with all participants.
Participants also discussed the redesigned VAC assistance service (1-800-268-7708):
- it is a free, confidential, 24/7 resource, available to all Veterans (not just VAC clients) and their family members
- operators are all mental health clinicians, trained to do a brief telephone assessment of the issues the caller wants help with, and then to refer to a health care provider in the Veteran or family member’s own community, for up to 20 face-to-face sessions of counselling.
All participants agreed that Veterans’ spouses or parents were often key in convincing an individual to seek care, and because of this they should:
- be given R2MR training to develop the necessary skills to deal with mental health issues
- know how to talk to their children and reduce the risk of legacy issues
- have access to treatment and diagnosis in their own right.
Outreach
Participants mentioned that outreach efforts are necessary and require:
- working with health professionals and local communities
- follow-up with health care professionals when a Veteran is at risk
- tracking and identifying Veterans in crisis, who are homeless or in the justice system
- further collaboration with the provinces.
Next Steps
- After the consultation phase, the VAC/CAF strategy will be completed, taking into consideration feedback received from Mental Health Advisory Group members.
- A VAC suicide prevention Action Plan will be developed, based on the Strategy, and will be updated on an ongoing basis as new evidence becomes available.
Presentation: Mental Health Commission of Canada (MHCC)
The presenter described suicide as a multifaceted issue that needs a whole-of-community intervention, tailored to each unique community. Key elements of reducing rates of suicide in communities include:
- Training for specific individuals, gate keepers, police, physicians, employers, school teachers, sports coach, on how to look for indicators and signs suicidality.
- Awareness: general awareness for the public, R2MR training, awareness in schools, guidelines on how the media reports on suicide
- Restricting means at the community level, including but not limited to railway crossings, educating pharmacists, etc.
- Research: access to data, evaluating outcomes, identifying high risk populations
- Supports: for those individual at-risk groups.
Member warned that the suicide prevention strategy on its own will not achieve the results if it is not linked to the provinces, different communities and diverse audiences (aboriginal, paramedics, health professionals, LBGTQ etc.).
Presentation: Mood Disorders Society (MDS)
The MDS has developed a Post-Traumatic Stress Disorder (PTSD) continuum to recognize, diagnose, and treat individuals.
Recommendations for suicide prevention:
- expand programs, focus on health care providers and improve funds to promptly address mental health issues
- Fund peer support programs and provide Veterans with peer support training
- Destigmatize mental health issues and raise awareness within the general population
- Include information from the Standing Committee on Veterans Affairs (ACVA) meetings in MDS recommendations.
Members noted that:
- mental illnesses are deceiving and peers need to be educated on recognizing the signs
- postvention becomes important and can answer “what did I miss?”
- triaging intervention in the medical field can sometimes increase stigma
- in grieving, communities need to recognize instead of sensationalize suicide.
Presentation: Prevention of Suicide – Princess Patricia Canadian Light Infantry (PPCLI) Association
- PPCLI Association is a volunteer-based organization, established in 1917
- It has 15 branches across Canada and a large online presence
- The Association provides feedback, assistance, coordinated support, fitness, comradeship, sense of purpose, leadership
- The organization has observed an increased rate of suicide among Veterans (post-release)
- The organization believes suicide prevention should be community based, support effective transition, and include proactive outreach and follow-up
- While not mental health specialists, peer-support groups such as the PPCLI Association can offer other support and personalized follow-up: drive a member to treatment, a kind ear, other activities.
Participants observed that peer-support groups should:
- remember their unique role
- educate themselves with appropriate training
- be mindful in achieving a balance and taking care of themselves.
Next Steps
- Advisory Group input into the suicide prevention strategy on an ongoing basis, as requested and continued information sharing with VAC and CAF/DND.
- Improved communication and provision of information to Advisory Group members.