
Table of contents
- This publication is available upon request in alternate formats.
Executive summary
Program profile
The Research and Innovation Program, formalized in 2019, supports Veteran health and well-being through evidence-based research and knowledge mobilization. It consists of five subcomponents:
- The Centre of Excellence on Post-Traumatic Stress Disorder and Related Mental Health Conditions (now the Atlas Institute for Veterans and Families)
- The Chronic Pain Centre of Excellence (CPCoE)
- Operational funding for the Canadian Institute for Military and Veteran Health Research (CIMVHR)
- The Joint Federal Research Funding Program (JFRFP)
- The Veteran and Family Well-being Fund (VFWF)
Together, annual expenditures for the program were approximately $25.5 million in 2024–25.
Evaluation purpose and background
The evaluation was conducted between September 2024 and September 2025 and assessed the program’s relevance, performance, and efficiency for the period April 2019 to March 2025. It examined continued need, alignment with federal priorities, achievement of intended outcomes, and opportunities for improvement. The evaluation used multiple lines of evidence, including document review, interviews with over 50 stakeholders, and analysis of operational and financial data. The VFWF was scoped out of the evaluation as it was evaluated separately in 2023.
Evaluation findings
The evaluation confirms a sustained need for Veteran and family-focused health research, particularly in the areas of chronic pain and mental health. Since 2019, more than 100 research projects have been supported as a result of program funding, reflecting the growing demand for evidence-based insights to enhance awareness and inform clinical practices and policy.
Program objectives remain aligned with Government of Canada priorities and the mandate of Veterans Affairs Canada (VAC). Established objectives are shaped by the lived experiences of Veterans, ensuring that research efforts are relevant and responsive to real-world needs. The evaluation identifies an opportunity to review and clarify the role and mandate of the department in research linked to first responders.
Performance across program sub-components was measured primarily against indicators in the program’s established performance information profile. The evaluation identifies information is being captured and reported, however there are inconsistencies and opportunities to improve the performance metrics. The performance indicators used by VAC to measure program success predominantly measure program reach versus impact. And, in the case of the JFRFP, performance indicators have not yet been developed, limiting the ability to assess its impact. The CPCoE and the Atlas Institute have met or exceeded targets for partnerships, knowledge products, and audience reach. Citation rates for research studies are increasing, indicating strong uptake of their work. CIMVHR is also on pace to meet expectations, as they continue to expand partnerships and journal reach grows.
Knowledge mobilization emerged as a recurring theme throughout the evaluation. Although all program subcomponents emphasize dissemination, there is no centralized repository or formal mechanism to ensure research flows to VAC. This reduces the potential for research to inform VAC policy and program development improvement.
From an efficiency perspective, program funds are spent with minimal lapse. However, sustainability risks exist due to the reliance of the centres of excellence on VAC as their sole funder. The decreasing value of annual fixed contribution amounts over the contribution period is also a risk for both the centres of excellence and CIMVHR. These factors may constrain the ability of funded organizations to continue to meet objectives and/or adapt in the future. Overall, the Research and Innovation Program expenditures account for less than half a percent of total departmental program expenditures.
Based on these findings, the evaluation identifies the following recommendations:
Recommendation #1
The Assistant Deputy Minister Strategic Policy, Planning and Performance and the Assistant Deputy Minister of Service Delivery review and update the current Research and Innovation Program Performance Information Profile to:
- develop and implement performance indicators to measure success of the Joint Federal Research Funding Program; and
- enhance conciseness and consistency of performance measures and methodologies across the program sub-components.
Recommendation #2
The Assistant Deputy Minister Strategic Policy, Planning and Performance develop a departmental knowledge mobilization plan, including how externally funded research is funneled back into VAC to support program management and policy development.
1.0 Introduction
Veterans Affairs Canada (VAC) has a mandate to support the well-being of Veterans and their families and to promote recognition and remembrance of the achievements and sacrifices of those who served Canada during war, military conflict, and peace. As part of this mandate, VAC receives funding to advance research and innovation related to Veteran health and support needs.
The Research and Innovation Program, formalized in 2019, originated from a 2015 commitment to expand the evidence base on Veterans’ health needs. The program currently consists of five subcomponents:
- Veteran and Family Well-being Fund (VFWF)
- Centre of Excellence on Post-Traumatic Stress Disorder and Related Mental Health Conditions (now the Atlas Institute for Veterans and Families)
- Chronic Pain Centre of Excellence (CPCoE)
- Funding for the Canadian Institute for Military and Veteran Health Research (CIMVHR)
- Joint Federal Research Funding Program (JFRFP)
Together, these subcomponents represented approximately $25.5 million in annual expenditures in 2024-25.Footnote 1
The Research and Innovation Program serves as an overarching framework that encompasses several subcomponents, each of which was launched at different times and under distinct authorities. Figure 1 illustrates the hierarchical structure of the Research and Innovation Program, including its subcomponents and associated terms and conditions. Notably, three of the components are grouped under the Research Funding Program for the purposes of funding authority and reporting.
Figure 1 – Research and Innovation Program authority structure and funding
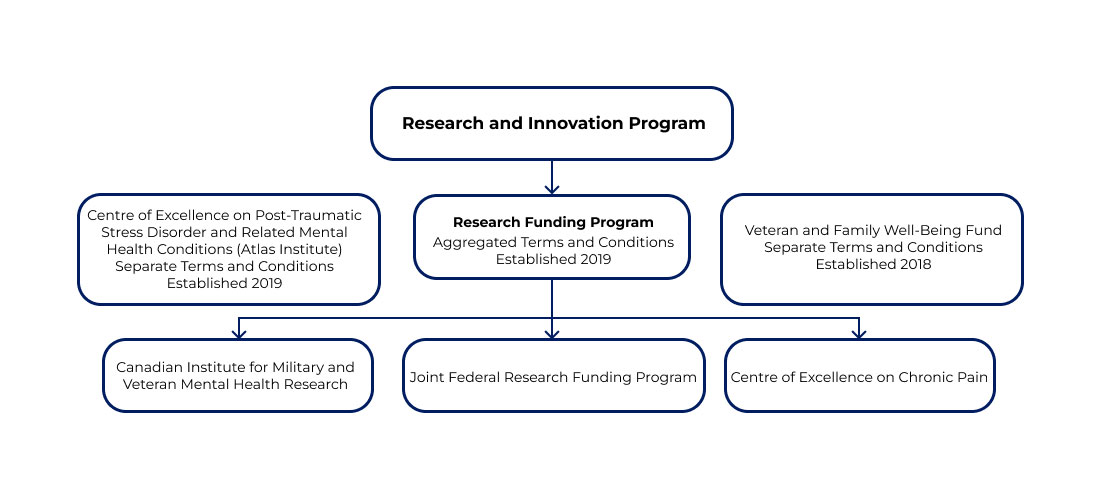
Transcript - Figure 1
Diagram showing the Research and Innovation Program authority structure and subcomponents. The diagram shows that CIMVHR, the JFRFP and the CPCoE are grouped together as part of the Research Funding Program which falls under the Research and Innovation Program umbrella. It also shows that the Atlas Institute and the VFWF are separate programs that still fall under the umbrella of the Research and Innovation Program.
1.1 Overview Veteran and Family Well-being Fund
The Veteran and Family Well-Being Fund (VFWF) was created in 2018 to fill an identified gap in supporting innovation and research for Veteran health and well-being. Prior to establishing the fund, VAC regularly received requests from organizations to support research and/or the development of programs and services for Veterans and their families. The Department, however, had no formal mechanism to contribute financially to these requests.
The intent of the VFWF is to provide financial support to organizations that conduct research and/or develop/implement innovative programs and services intended to improve the health and well-being of Veterans and their families. The fund can support a wide range of projects such as suicide prevention research, homelessness research, or any innovative projects that contribute to Veteran/family well-being.
The fund can provide:
- grants up to $500,000 per fiscal year for eligible projects; and
- contributions of up to $1 million per fiscal year for larger research initiatives.
The VFWF has a base annual budget of $3 million and has had several infusions of temporary funding, most recently through Budget 2024.Footnote 2 A portion of the funding focuses on projects for Indigenous, women, and 2SLGBTQI+ Veterans.
1.2 Overview of the Centre of Excellence on Post‑Traumatic Stress Disorder and Related Mental Health Conditions (now the Atlas Institute for Veterans and Families)
The 2015 VAC mandate letter from the Prime Minister identified, as a top priority, the creation of a centre of excellence with a specialization in mental health, PTSD, and related issues for Veterans and first responders.Footnote 3 The objective of forming a centre of excellence was to increase the Canadian expertise, knowledge creation, and transfer of knowledge on the subject of mental health, suicide prevention and substance use disorders. This mandate was timely given the sharp increase in approved disability applications for mental health conditions between 2020 and 2025 (more than 350% increase).Footnote 4
Operational since April 2019, and rebranded in 2022 as the Atlas Institute for Veterans and Families (hereafter referred to as the Atlas Institute), the organization brings Canadian Armed Forces (CAF) and Royal Canadian Mounted Police (RCMP) Veterans, first responders, families, service providers, and research partners together to create, gather and share knowledge on Veteran and family mental health. The Atlas Institute also helps integrate this information into practice to improve treatment and support.
The Atlas Institute is affiliated and co-located with the Royal Ottawa Mental Health Centre.Footnote 5 The Royal is a teaching and research hospital that provides mental health care. This partnership provides the Atlas Institute with access to specialized equipment for research purposes (e.g., brain imaging technology) and administrative support.
VAC currently provides $9.2 million annually to the Atlas Institute under a 2022-23 to 2026-27 contribution agreement ($46 million total).
1.3 Overview of the Centre of Excellence on Chronic Pain
The 2015 mandate letter that called for the development of a centre of excellence on PTSD also instructed the department to develop a second centre of excellence to be identified based on departmental priorities. VAC looked to the results of the VAC Life After Service Survey (LASS)Footnote 6 to provide insight into areas of greatest need. The survey determined that Veterans were twice as likely to experience chronic pain compared to the general Canadian population, with over 40% of Veteran respondents reporting suffering from chronic pain. This data was a key driver informing the decision to focus on chronic pain.
In 2020, the Chronic Pain Centre of Excellence (CPCoE) was established as a research centre to improve the understanding of Veteran-specific chronic pain and how best to manage it. The Michael G. DeGroote Institute for Pain Research and Care at McMaster University in Hamilton, Ontario was named as the organization to set up the CPCoE.
The CPCoE partners with a network that includes academic research institutions and other organizations across the country that focus on chronic pain research and pain management. The organization allocates research funding through a competitive application process, which includes review by a Scientific Advisory Board. In addition to project funding, the CPCoE provides capacity-building support for graduate students through its Capacity Building Initiatives (CBIs). These initiatives are intended to foster research in areas related to chronic pain among Veterans.
VAC currently provides the CPCoE with $4,661,679 annually under the terms of a contribution agreement that runs from 2023-24 to 2027-28 ($23,308,395 total). The funding is to be used for operational expenses including salaries, rent, utilities, travel, supplies, etc.Footnote 7
1.4 Overview of Canadian Institute for Military and Veteran Health Research
The Canadian Institute for Military and Veteran Health Research (CIMVHR) was launched in 2010 to engage existing academic research resources and facilitate the development of new research, research capacity and effective knowledge translation. With a network of academic researchers from across Canada, the Institute serves as a focal point for 46 Canadian universities who have agreed to work together in addressing the health research requirements of the Canadian military, Veterans, and their families. The institute acts as a conduit between the academic community and research funding organizations (both public and private).
The institute was founded through the combined involvement of Queen’s University, the Royal Military College, and the Surgeon General’s office. Its key areas of focus include mental health, rehabilitation, post-service transition, military families, and operational health.
CIMVHR key activities include:
- an annual Forum which serves as a platform for researchers, academics, and stakeholders across various sectors to exchange insights, collaborate, and showcase advancements in research and ideas for the betterment of military personnel, Veterans and their families (900 participants in 2024)
- the publication of The Journal of Military, Veteran and Family Health (JMVFH), an online, open access, peer-reviewed scholarly journal that was first published in 2015 (approximately five issues per year)
- the establishment of partnerships and networks to help drive research and knowledge translation on Veteran and military health
- the distribution of requests-for-proposals to researchers through CIMVHR’s network of universities and the management of the task through the scientific peer-review process to the completion of the project
- the administration of post-graduate scholarships aimed at building research capacity within the field of Veteran and military health
CIMVHR’s operations were originally funded through a contribution agreement with Health Canada. Though VAC has partnered with CIMVHR since its inception, the Department formally entered into a funding agreement with the organization after an announcement was made in Budget 2019.Footnote 8 VAC signed a formal agreement to support CIMVHR’s operational activities for 10 years (2020-21 to 2029-30) at an annual expenditure of $2.5 million ($25 million total).
1.5 Overview of the Joint Federal Research Funding Program for Military Personnel and Veterans
In 2023, VAC launched the Joint Federal Research Funding Program for Military Personnel and Veterans (JFRFP). The program aims to enhance the well-being of CAF members, Veterans, and their families by supporting Canadian research focused on supporting these populations. The program is a partnership between VAC and:
- the Canadian Forces Health Services Group (CFHS);
- Defence Research and Development Canada (DRDC); and
- the Canadian Institute for Military and Veteran Health Research (CIMVHR).
The JFRFP replaces a previous model where research activities were conducted through a contract-based task authorization process.Footnote 9 Under that approach, CIMVHR held a task agreement with PSPC to support research for DND and VAC.
The objectives of JFRFP are to:
- drive progress on new knowledge and understanding of military members, Veterans and well-being of their families;
- foster the development and implementation of policies and strategies on programs and benefits that address identified priorities for Canadian Armed Forces members, Veterans and their family well-being;
- identify, assess, and promote new approaches, models, and best practices, leading to improved well-being for military members, Veterans and their families;
- build capacity within the research field engaged in studying Veterans’ issues; and
- foster partnerships and networks with research institutions
Organizations eligible for funding through the JFRFP include:
- non-profit, educational, research, public health, and social services institutions;
- provincial, territorial, and local governments;
- Indigenous and international non-profit organizations;
The fund may be used for research activities such as: literature reviews; surveys; experimental and clinical studies; field studies and data analysis; population statistics; workshops and presentations to government and health care system stakeholders; and the development of tools and treatments.
Under the terms of a 2023 Memorandum of Understanding (MOU), VAC, DND, and the CAF are funding partners in the program and are to each contribute a minimum of $500,000 per year for funded projects. DND and the CAF, through DRDC and the CFHS Group respectively, will also each contribute $50,000 per year plus 4.25% of the value of their respectively sponsored projects for VAC to administer funding competitions and funding agreements relating to those projects.Footnote 10
Both DRDC and CFHS transfer funds to VAC through Annual Reference Level Updates (ARLU) or Supplementary Estimates, as appropriate. Funds transferred to VAC are to be equal to the value of the projects respectively sponsored by each funding partner, plus sufficient funds for VAC to administer research funding competitions and any resulting project funding agreements. Calls for research proposals are disseminated through CIMVHR’s network of research partners, with successful candidates receiving funding through a grant or a contribution (to date, only grant funding has been awarded).
2.0 Scope and methodology
2.1 Evaluation objective and scope
This evaluation was conducted in accordance with VAC’s 2024-25 to 2028-29 Departmental Evaluation Plan, which was developed to align with Treasury Board’s 2016 Policy on Results. The evaluation fulfils policy requirements and Financial Administration Act requirements to evaluate:
- VAC programs with annual expenditures averaging more than $5,000,000 per year; and
- organizational spending on programs in the department's program inventory based on risk or need.
Evaluation coverage and criteria under the Policy on Results requires that the past performance and current activities of the Research and Innovation Program be reviewed to determine program relevance, effectiveness, and economy. Program expenditures for the umbrella Research and Innovation Program exceed $5 million annually, though individual components by themselves may not meet this threshold.
The past performance of the program was reviewed along with current activities to determine program relevance, effectiveness, and economy. Analysis conducted while planning the scope for the evaluation indicated that program relevance to VAC’s mandate and knowledge mobilization were underlying themes that needed to be reviewed.
The evaluation launched in September 2024 and was substantially completed by September 2025. A draft report was completed by October 2025 and presented to the Performance Measurement and Evaluation Committee (PMEC) for recommendation December 2025. Final report approval was received in January 2026. The evaluation covers the period from April 1, 2019 to March 31, 2025. When available and applicable, more up-to-date statistics and information was incorporated into this evaluation report.
Early in the evaluation planning process, the Veterans Family and Well-being Fund component was scoped out as it was evaluated separately in 2022-23. Reference may be made to the VFWF within this report as VAC human resources dedicated to administer this program component within VAC’s Research Directorate also have responsibility for the JFRFP. VAC’s Research Directorate as a whole and its role in conducting primary and secondary research was not evaluated, though reference is made within the report to set the historical context of Veteran health research in Canada.
Other scoping notes regarding the evaluation conduct include:
- initial grants from VAC to establish (i.e., make operational) the Atlas Institute and the CPCoE were not examined;
- day-to-day/internal operations of the funding recipient organizations were not assessed, as the recipients are arms-length/independent organizations; VAC’s relationship with CIMVHR prior to 2020 was not considered in scope, as it was not within the Research and Innovation Program;
- JFRFP program performance was not examined as only one VAC research project had been completed at the time the evaluation was conducted. The evaluation focussed on relevance and economy for this program component; and
- while VAC collaborates with DRDC and CFHS in administering the JFRFP, this evaluation focused primarily on the program’s implementation and impact from VAC’s perspective.
2.2 Evaluation questions
Upon completion of an initial review (interviews, document review, and data analysis), evaluation questions were developed under the themes of relevance, performance and efficiency/economy to help assess the Research and Innovation Program. Evaluation questions highlighting the key lines of inquiry can be found in Table 1 below:
Relevance
- To what extent does the Research and Innovation Program address a need for Veteran health research and knowledge mobilization?
- To what extent do the program components align with Government of Canada priorities and departmental roles and responsibilities?
Performance
- To what extent does the program design facilitate the achievement of the Research and Innovation Program objectives?
- To what degree is the Research and Innovation Program achieving intended outputs and outcomes?
- Are there any unintended impacts resulting from the Research and Innovation Program (positive or negative)?
Efficiency/Economy
- To what extent is the program being effectively and efficiently delivered?
2.3 Evaluation methodology
The Evaluation was summativeFootnote 11 in nature and relied on a mix of qualitative and quantitative data sources. The methodology incorporated multiple lines of evidence to ensure reliability of collected information and reported results. This information is further outlined in Table 2 below.
| Methodology | Source |
|---|---|
| Departmental Documentation and Secondary Research Review | The following Departmental documents/information were reviewed to understand the program objectives/intent, their authorities and requirements, complexity, context, and key issue areas: internal planning documents, central agency submissions, contribution agreements, memorandums of understanding, previous audits and/or evaluations, records of decisions, strategic documents, performance reports, and research papers. |
| Non-Departmental Document Review | Various non-departmental documents such as, parliamentary reports and transcripts, legislation, budget speeches, industry research, media documents, and Speeches from the Throne were reviewed for context purposes. Documentation, reports, and studies produced or sponsored by the centres of expertise, CIMVHR, and through the JFRFP were also reviewed. |
| Interviews | Interviews were conducted with more than 50 subject matter experts including: VAC senior management, past program managers, policy managers, and research staff; Atlas Institute staff and management; CPCoE staff and management, CIMVHR staff and management; and program managers at DND/CAF. |
| Data Analysis | Analysis was conducted of VAC operational data and financial data pertaining to the Research and Innovation Program since its launch April 1, 2019. |
2.4 Considerations and limitations
The evaluation identified the following considerations and limitations:
- The evaluation team consulted with VAC staff and staff from the various program components/organizations to gain an in-depth understanding of workflows, activities, and operations to help determine what is working well and where there may be areas for improvement with regards to the Research and Innovation Program. During the planning phase, the evaluation team also conducted site visits at organizations who have funding agreements with VAC through the Research and Innovation Program (the Atlas Institute, the CPCoE and CIMVHR). It was not possible to conduct in-person interviews with all individuals due to available resources and geographic locations. Virtual consultations were conducted in some situations.
- Certain components of the program have existed longer than others. The amount of operational data and performance measurement data available varied between components.
- Research results take time and may not yet be contributing to the program’s intermediate or ultimate outcome. Where ultimate results have not yet been realized, the evaluation will focus on whether there are measures of success in place to determine/guide future program success. The evaluation team reviewed available quantitative output data as well as qualitative feedback collected by organizations from stakeholders/participants.
- The Atlas Institute, CIMVHR, and the CPCoE are independent organizations and as part of their funding agreement there is a requirement for an external third party review. A third party review of CIMVHR operations occurred in the spring of 2025. The evaluation team took findings from the review report into consideration during document review.
- The Department’s internal Research Directorate and its activities were not considered in scope of the evaluation as they are not included within the Research and Innovation Program.
The above noted information should be taken into consideration when reading this evaluation report. Additional limitations may be identified throughout the report where applicable.
3.0 Relevance
Veterans Affairs Canada has a mandate to promote the well-being of Veterans and their families. The components of the Research and Innovation Program were developed to support this mandate by facilitating partnerships, research and knowledge mobilization activities that contribute to evidence-informed health strategies and, ultimately, improved outcomes for Veterans.
3.1 Need for the Research and Innovation Program
Research on Veterans’ health is essential to understand and address the unique physical, psychological, and social challenges that arise from military service. Veterans often experience conditions that differ in nature, frequency, or severity from those in the general population, such as operational stress injuries, chronic pain, and service-related disabilities. These health issues can emerge years after service, change over time, and affect not only Veterans but also their families. Evidence-based research provides a foundation for effective policies, programs, and treatments, ensuring that support systems are responsive to evolving needs. Without ongoing, targeted research, gaps in care may not be identified and addressed, leading to poorer outcomes for Veterans.
Evolution of Veteran health research
Historically, VAC conducted extensive in-house research through its hospital network, employing more than 100 research staff in the 1950s and reporting 90 active studies by 1962. This capacity declined in the 1970s and 1980s following as the federal government began transferring federal health facilities to provincial control.
As the health needs of Veterans have evolved, particularly with emerging challenges among younger CAF Veterans, VAC identified the need to enhance national research capacity. While the Department’s internal Research Directorate contributes to evidence generation and analysis, it has limited resources to address the full range of research required to support Veteran well-being and foster national and international partnerships.
To expand Veteran health research capacity, VAC invests in external organizations that complement its internal work:
- CIMVHR serves as a hub for military and Veteran health research, connecting VAC with a broad evidence base and academic institutions across Canada;
- Both CPCoE and the Atlas Institute focus on specific areas of need (chronic pain and mental health) while operating at arm's length to maintain independence and alignment with VAC priorities; and
- JFRFP and the VFWF enable VAC to support targeted projects and focus research priorities on emerging issues.
These investments allow VAC to access a diverse body of research to inform policy, improve programs, and support outcomes for Veterans and their families. This approach reflects a transition from only conducting research internally to leveraging national research capacity.
3.1.1 Initial rationale for program components
The evaluation team examined the rationale for the various subcomponents of the Research and Innovation Program to determine if they address areas of need within the Veteran population and whether they addressed capacity gaps within the department (see Table 3).
| Component (topic/focus area) | Rationale | Additional supporting evidence |
|---|---|---|
| Atlas Institute (mental health) | 2015 Mandate Letter which instructed VAC to create two new centres of excellence in Veteran’s care, including one with a specialization in mental health, post-traumatic stress disorder and related issues for both Veterans and first responders. | From 2020-21 through 2024-25, approximately 30% of disability first applications approved by VAC had at least one mental health related medical condition and more than 50,000 Veterans (50%) are receiving disability benefits for mental health conditions.Footnote 12 |
| CPCoE (chronic pain) | To improve well-being outcomes for military members, Veterans, and their families, focused research is required to better understand the role of military service in causing chronic pain and to identify the best, evidence-based treatment alternatives for this population. 2015 Mandate Letter instructed VAC to create a second centre of excellence and 2017 Mandate Letter further elaborated it should be based on the area of greatest need. | Forty-one percent (41%) of Veterans have chronic pain, more than double the incidence in the Canadian population. Research demonstrates that chronic pain is common in persons with musculoskeletal disorders. Departmental data from March 2025 shows that 64,371 of Veteran clients (63%) were receiving disability benefits for musculoskeletal disorders. |
| CIMVHR (academic and global research affiliations) | In providing funding for CIMVHR’s operations, a link between VAC and leading researchers across Canada will be created to support collaboration on research projects related to the health and well-being of the military, Veterans and families. In addition, links to the academic community and researchers from different countries will support VAC in its collaboration on international and multi-disciplinary projects. | Prior to VAC funding in 2020, CIMVHR had developed a network of 45 Canadian universities, 12 global affiliates, and more than 1,700 researchers, that agreed to work together in addressing the health research requirements of military members, Veterans, and their families. |
| JFRFP (interdepartmental research) | Memorandum of Understanding that outlines the provisions under which the Participants collectively fund research related to military members, Veterans, and their families through the VAC Research Funding Program. | Research capacity gap at CFHS and DRDC resulting from the end of task authorization contracting. VAC had the authority to administer a grant and contribution program to meet outstanding research needs. VAC proposed a joint research fund as a responsive solution to collaborate and meet research needs at all three organizations. |
The need for both centres of excellence and CIMVHR is supported by mandate letters, Treasury Board submissions, and data demonstrating the prevalence of chronic pain and mental health conditions among Veterans.
3.1.2 Continued and ongoing need
Departmental operational data indicates a consistent increase in the number of clients receiving disability benefits for mental health conditions since 2010, supporting the rationale for a centre of excellence on PTSD and other mental health conditions. Since 2020, the Department has approved an average of 7,033 first-time disability benefit applications annually that have at least one mental health-related condition. Similarly, the average number of first-time applications approved for a musculoskeletal condition in the same period was just under 7,000.
There is a strong correlation between mental health conditions and chronic pain, underscoring the relevance of integrated research efforts addressing both areas. Both musculoskeletal and mental health conditions are among the top ten medical conditions for which disability benefits are awarded.
The evaluation team was unable to identify a baseline measurement of research activity existing prior to contribution funding through the Research and Innovation Program. As such, the evaluation team cannot quantify the precise change realized from program funding; however, between 2019 and September 2025, the evaluation team identified more than 100 research projects supported by the Atlas Institute, the CPCoE and CIMVHR. Examples of projects for each organization are provided in Appendices A through C.
The growing number of completed projects, and strong participation in training sessions, webinars, and conferences/summits organized by the centres of excellence and CIMVHR indicate a need for research information and supporting resources and training (see Section 4.1 for more information on audiences reached). As shown in Appendices A through C there is widespread demand for research funding across the country, as evidenced by the variety of institutions now conducting Veteran research.
The CPCoE addresses the disproportionately high incidence of chronic pain, the Atlas Institute focuses on mental health and PTSD, and CIMVHR facilitates national and international academic research collaboration. Finally, the JFRFP reflects a strategic approach to enhancing Veteran well-being through targeted research investment in military and Veteran health, though VAC’s use of the program to date has been minimal (discussed further in Section 4.1.4).
The evaluation team did not speak directly with stakeholder groups such as Veterans, their families, or clinicians. However, interviews with staff at VAC, the Atlas Institute, the CPCoE, and CIMVHR offered indirect insights, suggesting that Veterans and their families identify a continued need for health-related research, especially incorporating a lived experience lens. Several standing committees, including the Standing Committee on Veterans Affairs (ACVA) have also focused on military and Veteran health research. For example, ACVA issued a 2024 report recommending that VAC fund and carry out long-term research on servicewomen and women Veterans.
Although mandate letters were the main motivation for establishing the Centres of Excellence, the evaluation confirms through document review, data analysis and interviews that the subcomponents of the Research and Innovation Program align with identified research needs in key topic areas affecting military members and Veterans, and their families.
3.1.3 Priority setting
To further examine whether the direction of the centres of excellence align with the program intent, the evaluation team examined how the centres choose which research to undertake and whether it aligns with the overall priorities of VAC and the Research and Innovation Program.
Priority setting at CPCoE
The CPCoE was established and funded as an arms-length organization that has full autonomy from VAC in terms of the research it supports. Interviewees indicate this approach was intended to prevent any perception of bias and to alleviate skepticism about VAC’s influence on the Centre’s operations and research. Interviews with VAC staff point out that it was never the intention that the Centre conduct work on behalf of VAC nor does the contribution agreement indicate that research would be prioritized to meet VAC needs. As stated in Section 5.5 of the first funding agreement with McMaster University to create the CPCoE:
Similar wording has appeared in subsequent contribution agreements.
In terms of governance, annual CPCoE research priorities are established by a 15 member Advisory Council of Veterans (ACV). In 2023, the Centre initiated a form of the James Lind AllianceFootnote 14 evidence-based priority setting process that brings Veterans together with the ACV and researchers to develop research priorities, further enhancing the robustness of their planning process. See Figure 2 for an overview of the priority setting process.
Figure 2 – Chronic Pain Centre of Excellence Priority Setting Steps

Transcript - Figure 2
Diagram showing the CPCoE priority steps:
- Gathering issues of Relevance from Veterans, their families, clinicians, and Researchers.
- Evidence Checking to inform uncertainties
- Priority setting meeting - ACV prioritizes uncertainties
- Request for proposal development and publication based on identified priorities
Source: 2023 CPCoE Priority Setting Report
VAC does not control the CPCoE priority setting exercise by design as per the terms of the contribution agreement. The centre does, however, keep the Department informed about the topics it is researching and evidence suggests priorities often align (e.g., the recent focus on women Veterans). The CPCoE does take into consideration themes identified by VAC and open two-way communication exists.
Priority setting at the Atlas Institute
The Atlas Institute has developed a number of planning documents, including a strategic plan that highlights goals that align with the objectives identified in the contribution agreement. These goals can be categorized as:
- Prevention and preparation;
- Improved care and support;
- Engaging and informing; and
- Expanding what we know.
Similar to the CPCoE, the Atlas Institute’s priorities and strategic direction is guided by the lived experiences of Veterans and their families. The institute gathers feedback from various groups, including a strategic reference group composed of Veteran volunteers and their family members, service providers, and researchers. The Atlas Institute also collaborates with global leaders to inform research priorities, best practices, and to address emerging issues (e.g. Mental Health Research and Innovation Collaboration). Interviews with staff at both VAC and the Atlas Institute report a good relationship at the working level that enables communication between the organizations, including the opportunity to share the Department’s organization priorities.
The evaluation finds that both the CPCoE and the Atlas Institute have priorities that align with the goals of the Research and Innovation Program. Their focus on the health and well-being of Veterans and their families is reflected in central agency documents and their contribution agreements. These priorities are shaped through a process that considers Veterans’ lived experience.
JFRFP priority setting
The JFRFP continues to evolve. For example, roles and responsibilities and other process documents were being drafted during evaluation conduct. As part of the MOU, all three departmental partners meet on a regular basis to discuss research needs and to consider collaboration where possible. In terms of priority planning at VAC, interview feedback identifies that JFRFP research priorities are primarily aligned with departmental commitments and driven by senior management. A formal priority setting process was not in place at the time of the evaluation and research needs were determined on an ad-hoc basis.
3.1.4 Gender Based Analysis Plus
Gender-Based Analysis Plus (GBA Plus) is an analytical approach used to assess how diverse groups (including women, men, and gender-diverse individuals) experience policies, programs, and services. It considers multiple identity factors such as race, ethnicity, religion, age, and physical or mental disability. GBA Plus is integrated into the development of all VAC programs and benefits.
The evaluation team reviewed the sub-components of the Research and Innovation Program to determine how they incorporate GBA Plus principles in their activities and the research they support. The evaluation found that each sub-component incorporates GBA Plus considerations. Recipient organizations actively prioritize the inclusion of diverse populations when designing and conducting research projects. For example, each sub-component has supported research focused on women, contributing to the advancement of recommendations outlined in the 2024 ACVA report, "Invisible No More: The Experiences of Canadian Women Veterans".
Additional examples of consideration to GBA Plus factors can be found in Appendix D, Gender Based Analysis (GBA) Plus activity examples.
3.2 Alignment with Government of Canada priorities and federal roles and responsibilities
3.2.1 Alignment with Government of Canada priorities
The Department of Veterans Affairs Act provides authority to the Minister of Veterans Affairs to administer Acts of Parliament and Orders in Council that are not, by law, assigned to any other federal department or any Minister for the care, treatment and re-establishment in civil life of Veterans and the care of their dependents and survivors, and such other matters as the Governor in Council may assign. Two Orders in Council (2017 and 2019) give VAC authority to provide funding through the Research and Innovation Program.
Alignment with Government of Canada priorities and departmental roles and responsibilities is evident through two specific mandate letters from the Prime Minister to the Minister of Veterans Affairs:
- A 2015 mandate letter highlighted the creation of two new centres of excellence in Veterans care as a top priority. One centre was identified to focus on a specialization in mental health, post-traumatic stress disorder and related issues for both Veterans and first responders;
- A 2017 mandate letter further elaborated on the priority to establish two centres of excellence by stating a top priority to “implement the creation of a centre of excellence in mental health to enhance research and best practices and establish a second centre of excellence based on the area of greatest need.”
The 2017 and 2019 federal budgets proposed the creation of the centres of excellence, committing initial start up and ongoing funding to both centres. Additionally, language used in several federal budgets supports the intent of the Research and Innovation Program:
- Budget 2019 stated “It is our responsibility (Government of Canada) to ensure that all veterans and their families receive the support and services they need, when they need it.”;
- While not exclusive to Veterans or the evaluated programs, Budget 2022 included a focus on mental health, laying out government priorities and stating that “…the government will invest in identifying and expanding effective mental health interventions. …” ;
- Though linked to the Veteran and Family Well-being Fund, Budget 2024 prioritized supporting Veterans’ well-being and identified that Veterans’ organizations are often best placed to understand the needs of veterans.
Additionally, as highlighted in the 2020 Federal Framework on PTSD, the Government of Canada has the overarching role to provide information, foster partnership, support research and innovation, and undertake activities to promote and protect the physical and mental health of Canadians.
3.2.2 Alignment with departmental roles and responsibilities
The Research and Innovation Program supports departmental responsibilities. Though the Research and Innovation Program is not specifically named, the need to invest in research and/or increase understanding of Veterans’ physical and mental well-being is continually highlighted in VAC’s Departmental Plans from 2021-2022 through 2025-2026. For example, under the first core responsibility (Benefits, Services and Supports) the 2025-26 plan states “Support the care and well-being of Veterans and their dependents or survivors through a range of benefits, services, research, partnerships, and advocacy”.
The evaluation finds that the intent of the Research and Innovation Program serves to further the Minister’s mandate and departmental priorities and is aligned with departmental roles and responsibilities. However, the evaluation does note that the mandate established for the Centre of Excellence for Post-Traumatic Stress Disorder and Related Mental Health Conditions includes first responders in the target audience, which may not align with the mandate of Veterans Affairs. There is an opportunity to clarify the department’s role and responsibility as contribution agreements are reviewed and updated.
3.2.3 Potential duplication or overlap with other Government of Canada programs
Across the federal government, health research is largely centred in the federal health portfolio which includes Health Canada, the Public Health Agency of Canada and the Canadian Institute for Health Research (CIHR).
Canadian Institute for Health Research (CIHR)
CIHR is an independent agency that reports to Parliament through the Minister of Health. It was created in 2000 and is made up of thirteen virtual institutes, which focus on specific themes. The CIHR has no Veteran specific institute, however, there are potential similarities between the Atlas Institute and the CPCoE and CIHR institutes such as the Institute of Neurosciences, the Institute of Mental Health and Addiction, or the Institute of Musculoskeletal Health and Arthritis. Of note, while the CIHR institutes mainly focus on overall Canadian health themes/topics, there is a specific institute for Indigenous Peoples’ Health.
A review of available documentation indicates that while some research related to military personnel and Veterans is funded through CIHR, it represents only a small fraction of the total funded projects. A search of the CIHR database identified 17 relevant projects between 2020 and 2024, out of more than 18,500 research projects over the time span.Footnote 15 Although there is some potential for overlap or duplication, the limited scope of coverage, suggests that the risk is low. As such, the evaluation does not identify any immediate concerns.
Interviews with VAC staff indicated that consultations were held with other jurisdictions/organizations who created similar centres of excellence. Lessons learned were shared by these organizations that led the Department to the current grant and contribution funding model. The model emphasizes providing the centres of excellence with more independence and enhanced ability to be flexible and responsive to shifts in research. There is also a focus on growing research networks.
Canadian Institute on Public Safety Research and Treatment (CIPSRT)
CIPSRT was launched in 2018 as part of Public Safety Canada’s National Action Plan on Post-traumatic Stress Injuries by the Minister of Public Safety and Emergency Preparedness, in partnership with the Minister of Health.
CIPSRT has a similar mandate as the Atlas Institute, focussing on establishing and maintaining a network of researchers, post-doctoral fellows, and students working in the field of mental health research relating to public safety personnel. Working in partnership with the CIHR, CIPSRT has established a group to fund and mobilize research. Since its establishment, the organization has also expanded its scope to focus on RCMP. A review of both the Atlas Institute and CIPSRT websites identify statements and examples of collaboration/partnerships (e.g., convening a National Collaborative on PTSD and Related Mental Health Conditions). The evaluation team did not extensively review CIPSRT’s structure and research products. While collaborations are evident, the degree of similarities of mandates between CIPSRT and the Atlas Institute, specifically concerning RCMP, is an area VAC should consider when reviewing the contribution agreement with the Atlas Institute.
Federal Framework on Post-Traumatic Stress Disorder (PTSD)
The Federal Framework on PTSD, established under the 2018 Act and led by the Public Health Agency of Canada, provides a national approach to address PTSD among high-risk occupational groups. Its purpose is to strengthen knowledge creation, exchange, and collaboration across federal departments and stakeholders to inform evidence-based actions, reduce stigma, and improve recognition of PTSD symptoms and impacts. The framework also identifies ongoing initiatives and key partners, including military and Veterans, first responders, CIMVHR, the Atlas Institute, CIHR, and CIPSRT.
The framework’s guiding principle is intended to complement existing initiatives and leveraged partnerships. While there are no specific actions identified for VAC, the evaluation team notes that the Atlas Institute is identified as having a role in the framework as a lead in research, knowledge exchange and training. The framework priorities include:
- improved data on PTSD;
- promotion of clinical guidance and best practices;
- creation and distribution of education materials;
- strengthened collaboration.
The four priority areas in the framework align with the objectives of the Atlas Institute and CIMVHR and VAC goals and priorities around service excellence and data integrity.
The evaluation did not identify any specific duplication or overlap with other federal organizations/initiatives. However, as the research landscape continues to evolve, it is important to remain proactive. Future consideration for any departmental initiatives or funded organization priorities and/or initiatives should consider existing federal initiatives to avoid redundancy and strengthen alignment. Doing so will help maximize collaboration opportunities, leverage existing expertise, and ensure that departmental investments complement broader Government of Canada efforts rather than duplicate them.
4.0 Performance
The Research and Innovation Program was designed with the intent of expanding the field of Veteran research in support of Veterans, CAF members, and their families. The evaluation looked at the degree to which each subcomponent had performance metrics established to support effective measurement of intended outputs and outcomes, and to what degree information captured indicates progress or where there may be opportunities for improvement.
4.1 Effectiveness of the Research and Innovation Program
Measuring the impact of research is challenging; capturing outputs of studies and knowledge products is straightforward, but it is harder to make the leap to measuring impact on policy and/or treatments in the short term. Bibliometric analysis (including citations) is a common measurement of research reach and use.Footnote 16 Common methods to measure impact of research include: interviews/surveys with stakeholders and decision-makers, case studies, return on investment, logic models/theories of change and altmetrics.Footnote 17 Ultimately, impact can be measured by a change in health outcomes or health system processes/practices.
Supporting program performance structure
The Atlas Institute, the Research Funding Program,Footnote 18 and the VFWF are included within the Research and Innovation Program Performance Information Profile (PIP). Each has a corresponding logic modelFootnote 19 along with outcomes and performance indicators. In line with the evaluation scope, the evaluation team examined the PIP and logic models for the Atlas Institute and the Research Funding Program.
There is a degree of inconsistency in terms of the outcome statements and level of information captured and reported for the program components. For example, differing intermediate outcomes and the JFRFP falls under the Research Funding Program, but is not identified in the PIP. See Section 4.1.4 for more information on JFRFP performance measurement.
There are also inconsistencies in the methodologies. For example, “the number of audiences reached” is defined and tracked differently among the subcomponents (sometimes the number of events is tracked, sometimes individual attendance). Reviewing and adjusting methodologies and performance indicators/targets to enhance consistency would enable more thorough reporting and potential comparative analysis.
As the program sub-components have matured, some of the initial metrics for measuring program success need review. For example, the Atlas Institute, the CPCoE and CIMVHR all have as an immediate outcome that a network of partnerships be established. As of March 31, 2025, each organization has more than 40 partnerships, indicating that the networks have been established and therefore the immediate outcomes have been achieved.
4.1.1 Chronic Pain Centre of Excellence Performance
The purpose and objectives of the CPCoE have been modified slightly since the centre was founded. As per the terms of the 2020-2023 contribution agreement, the centre’s original purpose and objectives were to:
- drive progress on new knowledge and understanding of military member, Veteran and family well-being;
- foster the development and implementation of policies and strategies on programs and benefits that address identified priorities in military, Veteran and family well-being;
- identify, assess, and promote new approaches, models, and best practices, leading to improved well-being for military members, Veterans and their families;
- build capacity within the research field engaged in studying Veterans' issues; and
- foster partnerships and networks with research institutions.
The objectives under the 2023-2028 contribution agreement were modified to remove the focus on fostering development and implementation of polices and strategies on programs and benefits, in favour of:
- developing a strategy to track the number of Veterans annually receiving interdisciplinary care and collect data on the outcomes of interdisciplinary care of chronic pain in order to identify and share best practices.
- analyzing the effectiveness of programs and services that effect the well-being of Veterans suffering from chronic pain, and their families.
VAC has developed performance indicators specific to the CPCoE to help gauge the success of the Research and Innovation Program.
Performance indicators
Performance indicators for research can be generalized as measures of reach or measures of impact. Measures of reach attempt to capture who or how many are looking at information about research findings. This can be measured through various means including web page views, social media impressions, document downloads, podcasts listeners, and audience numbers at presentations. Reach indicators are useful to document and show progress is being made on the dissemination of research knowledge (knowledge mobilization). Measures of impact, however, attempt to address the question of whether the research is used or what effect it has had on outcomes.
As Table 4 and Table 5 show, performance indicators for the CPCoE’s immediate and intermediate outcomes relate mainly to reach rather than impact. Note that new targets were established at the conclusion of the first contribution agreement in March 2023.
| Indicator | Target 2020-2023 | Result | Status | Target 2023-2028 | Progress to March 2025 | Status |
|---|---|---|---|---|---|---|
| CPCoE partnerships established | 15 | 24 | Met | 45 | 19 | Exceeding |
Source: AED analysis of information on VAC’s Performance Outcomes and Indicators System (POIS).
| Indicator | Target 2023-2028 | Progress to March 2025 | Status |
|---|---|---|---|
| 1. CPCoE knowledge products distributed | 125 | 137 | Met |
| 2. Audiences reached by CPCoE through fora, workshops, etc. | 5000 | 188,172 | Met |
| 3. CPCoE research studies cited annually in grey or other literature to inform decision-makingFootnote 20 | 10% | 63% | Exceeding |
Source: Source: AED analysis of information on VAC’s Performance Outcomes and Indicators System (POIS).
The CPCoE reports quarterly to the department against its performance indicators and results are rolled up annually. The centre is on track to meet or exceed its partnership target by 2028 and has already fully met its 2028 target with respect to knowledge product distribution. This shows that the Centre is forming relationships and producing and sharing information effectively. However, the indicators do not speak to the types or quality of the partnerships being formed.
The measure of “audiences reached through events such as fora, workshops etc.” indicates 188,172 audience members compared to a target of 5,000. While this suggests broad outreach, the indicator needs to be refined as the definition of “audience” is not fully defined, making it difficult to determine whether the numbers reflect meaningful engagement or general exposure.
There is also an opportunity for VAC to enhance the PIP to reflect additional performance metrics around reach that provide a more fulsome picture of the CPCoE’s performance. For example:
- Research projects funded (76 research projects funded across eight Canadian provinces and Australia as of fiscal year 2024–25);
- Research projects completed (45 projects were completed as of 2024-25);
- Peer-reviewed articles published (28 peer-reviewed publications); and
- Types of partnerships (established partnerships with 30 universities and institutions).
The third intermediate indicator tracks how often CPCoE research studies are cited in grey or other literature to support decision-making. It shows a citation rate of 63% compared to a target of 10%. This is well above the expected level and suggests that CPCoE research is widely referenced. However, using citations alone as a proxy measure for impact has its limitations. While citations indicate visibility, they do not show whether the research influenced decisions or led to changes in practice, policy, or outcomes.
In 2024–25, the CPCoE implemented the use of Researchfish software to support the collection of data related to the impacts of funded research.Footnote 21 As part of this change, new reporting requirements were introduced for funding recipients. Researchers are now asked to submit progress reports through Researchfish, providing information on research outputs and outcomes. This includes details on publications (both grey and peer-reviewed), collaborations, engagement activities such as presentations and conferences, patient and public involvement, and any influence the research may have had on policy, practice, or other areas, including long-term impacts.
This approach is expected to enhance the availability and quality of data related to research impact, which will support future evaluations. As the CPCoE continues to develop its capacity to capture impact-related information, there may be an opportunity for VAC to revise intermediate outcome indicator #3 to better reflect the Centre’s evolving ability to measure research influence. As the CPCoE continues to mature, aligning performance measurement with its evolving activities and outputs will support more accurate and meaningful reporting on reach and impact.
Capacity building
As part of its Capacity Building Initiative, the CPCoE has provided support to 50 master’s and doctoral students. This initiative is intended to strengthen research capacity in the field of pain management by supporting graduate-level training and development.
Each year, the Capacity Building Initiative program may award funding to a maximum of two master’s students, each eligible for $27,000 annually over two years, and two doctoral students, each eligible for $40,000 annually over three years. A third Capacity Building Initiative was established in honour of a founding member of the CPCoE Advisory Council for Veterans. It offers an additional annual award of $27,000 to one francophone master’s student.
4.1.2 Atlas Institute Performance
The Atlas Institute was originally created to strengthen the capacity of individuals, organizations, and the healthcare community to understand and prevent the mental health impacts of trauma and PTSD on Veterans and their families and to improve recovery.
The formal funding agreement between VAC and the Atlas Institute outlines three key objectives focused on improving mental health outcomes for Veterans and their families:
- Enhancing expertise and sharing knowledge across the full continuum of care;
- Building new knowledge networks to connect research, evidence, policy, and practice; and
- Raising public awareness about mental health issues affecting Veterans and their families.
Performance indicators
The Atlas Institute has its own section within the Research and Innovation Program PIP. There are a total of 13 performance indicators tracked by VAC. Tables 6, 7a, 7b, 7c and 7d provide an overview of the immediate and intermediate program outcomes including: related performance indicators, available baseline measurements, targets, and results as of March 31, 2025.
| Indicator | Target 2019-2022 | Result | Status | Target 2022-2027 | Progress to March 2025 | Status |
|---|---|---|---|---|---|---|
| Number of diverse partnerships, collaborations and joint initiatives established | 15 (5 per year) | 25 | Exceeded | 15 | 15 | Met |
Source: AED analysis of information on VAC’s Performance Outcomes and Indicators System (POIS).
As can be seen in Table 6, the Atlas Institute has exceeded its past target for partnerships, and three years into its five year contribution agreement has already met the established target for that period. This would suggest a there should be a higher performance target set.
In addition to measuring the number of partnerships, there is a satisfaction indicator – percent of partners who report they are satisfied with the quality of their partnership with the COE on PTSD. This indicator was created in 2022 and the target is 75%. Results from 2022-23 through 2024-25 well exceeded the target, with over 93% of partners surveyed reporting satisfaction.
VAC has created several intermediate outcomes and related indicators to help monitor and evaluate the Atlas Institute’s performance (see Tables 7a, 7b, 7c and 7d).
Tables 7a, 7b, 7c and 7d: Atlas Institute Intermediate outcome performance measures
| Performance Indicator | Baseline (fiscal year) | Target (fiscal year) | 2020-21 | 2021-22 | 2022-23 | 2023-24 | 2024-25 |
|---|---|---|---|---|---|---|---|
| Number of large-scale applied research studies initiatedFootnote 22 | 0 (2022) | 3 (2027) | -- | -- | 3 | 3 | 4 |
| Performance Indicator | Baseline (fiscal year) | Target (fiscal year) | 2020-21 | 2021-22 | 2022-23 | 2023-24 | 2024-25 |
|---|---|---|---|---|---|---|---|
| Percent of research studies cited in grey or other literature to inform decision-making | 75% (2022) | 75% (2027) | -- | -- | 42% | 59% | 86% |
| Performance Indicator | Baseline (fiscal year) | Target (fiscal year) | 2020-21 | 2021-22 | 2022-23 | 2023-24 | 2024-25 |
|---|---|---|---|---|---|---|---|
| Percentage of satisfaction with the quality of the evidence‑based information and toolsFootnote 23 | 75% (2022) | 75% (2027) | -- | -- | 95%Footnote 24 | -- | 90% |
| Percent uptake of evidence‑based information products and tools | 80% | 80% (2027) | -- | -- | 100% | 100% | 100% |
| Performance Indicator | Baseline (fiscal year) | Target (fiscal year) | 2020-21 | 2021-22 | 2022-23 | 2023-24 | 2024-25 |
|---|---|---|---|---|---|---|---|
| Percent of VAC‑registered mental health service providers, trained by CoE, reporting application of CoE research findings | 75% (2022) | 75% (2027) | -- | -- | 89%Footnote 25 | -- | 75% |
Source: AED analysis of information on VAC’s Performance Outcomes and Indicators System (POIS). September 2025.
Note: several new performance indicators and outputs were established with the subsequent contribution agreement and some measurements are a cumulative count over the contribution period (i.e., the number of partnerships established within the contribution agreement period).
The established outcomes flow and are linked to the preceding intent and objectives outlined in departmental planning documents and the funding agreement with the Atlas Institute noted above.
In addition to the metrics presented in Tables 7a, 7b, 7c and 7d – Intermediate outcome performance measures, there are a number of other metrics captured. Additional performance information available is presented in Tables 8a, 8b and 8c. The evaluation team notes that some or all of these measures could be identified in the PIP as performance indicators in support of the above intermediate outcomes, which would be more in line with CPCoE.
Tables 8a, 8b and 8c – Performance outputs and indicators for the Atlas Institute
| Performance Indicator | Target (fiscal year) | 2020-21 | 2021-22 | 2022-23 | 2023-24 | 2024-25 |
|---|---|---|---|---|---|---|
| Number of knowledge products distributed Footnote 26 | 125 (2027) [25/year] | -- | -- | 27 | 29 | 25 |
| Number of audience members reached through fora, workshops, etc. | 750/year | -- | -- | 1,670 | 3,849 | 2,932 |
| Performance Indicator | Target (fiscal year) | 2020-21 | 2021-22 | 2022-23 | 2023-24 | 2024-25 |
|---|---|---|---|---|---|---|
| Number of research studies completed | N/A | 6 | 5 | 7 | 4 | 4 |
| Performance Indicator | Target (fiscal year) | 2020-21 | 2021-22 | 2022-23 | 2023-24 | 2024-25 |
|---|---|---|---|---|---|---|
| Number of training activities held /tools/educational products disseminated | N/A | -- | -- | 52 | 103 | 59 |
Source: AED analysis of information on VAC’s Performance Outcomes and Indicators System (POIS). September 2025.
Based on document review, the evaluation team identified an opportunity to enhance program outcomes. Specifically, combining the intermediate outcome statements into a single outcome focused on both the conduct and dissemination of research, while retaining multiple indicators, could improve clarity and alignment with program objectives. This change would link to all initiated research, while making the PIP more concise.
Many new performance indicators have been added since the establishment of the Centre, aiming to enhance foundational performance measures (as was shown in Tables 7a, 7b, 7c and 7d and Tables 8a, 8b and 8c, a number of measures were introduced in 2022-23). In 2024 the Atlas Institute produced its own Performance Measurement Framework with updated and suggested indicators and associated metrics, definitions, and targets. This was not a practice or document requested by VAC, but more an internal activity aimed to measured organization impact. There are over 50 indicators linked to a number of areas (mission, stakeholder, finances, and internal performance). While there is some overlap with VAC indicators (e.g. publications, partnerships, audiences reached/attendance), the Atlas Institute’s framework is more specific in nature and includes some operational/organization performance measures (e.g. organizational commitment and capacity, governance and leadership, and belonging). The evaluation notes there is an opportunity to expand the VAC PIP using performance information already collected by the Atlas Institute. For example:
- Initiated and active research studies (not just large scale applied research);
- Diversity of research studies initiated or completed (study topics/themes and study population);
- Average impact factor of publication journals (another common bibliometric that expands beyond measuring citations);
- Application of service provider trainings (service provider survey that applied training/learning in practice); and
- Addressing needs of veterans through engagement opportunities (number of participants and stakeholders that feel represented in the Atlas Institute’s work).
Performance-related information and output measurement is collected using various tools including partnership feedback surveys and Google Scholar (to track research impact). Evidence reviewed by the evaluation team demonstrates comprehensive reporting practices, and interviews indicate a strong commitment to improving and refining performance measurement.
Measuring the impact of research is a challenging endeavour; capturing outputs of studies and knowledge products is straightforward, but it is harder to make the leap to measuring impact on policy and/or treatments in the short term. There is an opportunity to capture and report on qualitative impact realized from partnerships and/or research projects, for example the evaluation has seen qualitative evidence of impact through testimony presented at an ACVA standing committee.
While they are still in early growth stages, the Atlas Institute has contributed to the evidence base on mental health research related to Veterans and their families through consistent completion of research studies (Tables 8a, 8b and 8c) that have seen a steady growth in the frequency of citations (Tables 7a, 7b, 7c and 7d). Between 2022-23 and 2024-25, there were 27 studies completed. Bibliometric analysis conducted by the Atlas Institute shows that 86%of the studies were cited as of March 31, 2025. Further complementing this research, information shared by the Institute indicates consistent distribution of knowledge products that exceeds their target for audience reach.
Bibliometric analysis (including citations) is a common measurement of research impact used by other federal government departments that are funding research. Other common methods to measure impact of research funded include:
- interviews/surveys with stakeholders and decision-makers;
- altmetrics (e.g. social media and public engagement);
- return on investment and/or cost savings; and
- logic models/theories of change.
Ultimately, impact would be measured by a change in health outcomes and/or health system processes/practices.
Capacity building
Capacity building can be considered from a number of perspectives – health care practitioners, Veterans and their families, and the research community. The Atlas Institute’s strategic focus includes improving care and support, with an emphasis on increasing capacity across Canada for accessible, culturally competent and trauma-informed care and support. In this respect, the target is primarily service providers, Veterans and their families. The organization currently measures audiences reached, activities held/tools created and information downloaded from their website.
As the Atlas Institute advances research capacity in Canada, there is an opportunity to monitor its impact on the research community. For instance, the proportion of projects that include early-career or student researchers could be tracked. Such a performance indicator would be consistent with the Institute’s mandate and key activities, which include positioning the Centre of Excellence as a national/international leader in PTSD research that creates opportunities to support the the next generation of researchers from a diversity of horizons.
Overall, there is a significant amount of performance related information available to VAC. While much of it is output and reach oriented, there are opportunities to considering incorporating more performance indicators into the current PIP to provide a more fulsome performance picture of the results.
4.1.3 Canadian Institute for Military and Veteran Health Research Performance
CIMVHR falls under the Research Funding Program section of the PIP. Tables 9a, 9b and 9c provide an overview of the related performance indicators, including targets and results as of March 31, 2025.
Tables 9a, 9b and 9c – CIMVHR Performance Indicators
| Performance Indicator | Baseline (fiscal year) | Target (fiscal year) | 2020-21Footnote 27 | 2021-22 | 2022-23 | 2023-24 | 2024-25 |
|---|---|---|---|---|---|---|---|
| Number of partnerships established by CIMVHR | 60 (2020) | 87 (2026*) | 62 | 69 | 70 | 74 | 78 |
* target date was initially set for March 31, 2024, but has been deferred to March 31, 2026.
| Performance Indicator | Baseline (fiscal year) | Target (fiscal year) | 2020-21Footnote 27 | 2021-22 | 2022-23 | 2023-24 | 2024-25 |
|---|---|---|---|---|---|---|---|
| Number of CIMVHR knowledge products distributed | 40 (2021) | 21 (annual) | 40 | 90 | 21 | 25 | 65 |
| Number of audiences reached by CIMVHR through fora, workshops, etc. | 9 (2021) | 10 (annual) | 9 | 14 | 5 | 11 | 20 |
| Performance Indicator | Baseline (fiscal year) | Target (fiscal year) | 2020-21Footnote 27 | 2021-22 | 2022-23 | 2023-24 | 2024-25 |
|---|---|---|---|---|---|---|---|
| Number of annual article downloads from CIMVHR’s Journal of Military, Veteran and Family Health | 148,133 (2022) | 165,000 (2026) | 78,381 | 103,969 | 148,133 | 157,101 | 182,098 |
Source: POIS, Research and Innovation Program PIP Results. As of July 2025.
To drive research and knowledge translation, CIMVHR has grown its partnerships and networks. At the outset of the funding agreement in 2020, the organization had 60 partnerships with an aim to grow this base to 87 by 2024. In 2023-24, due to staffing considerations and a re-emphasis on strategic priorities, CIMVHR began to focus on improving the quality of existing relationships over establishing new ones. The organization plans to continue to grow their partnership base in the coming years.
In addition to expanding partnerships, CIMVHR contributes to the Research and Innovation Program by developing a range of knowledge products. As shown in Tables 9a, 9b and 9c, the number of products was notably higher in 2021–22 (90), due in part to a virtual Forum that featured a large number of streamed video presentations.
CIMVHR’s flagship event, annual Forum, draws hundreds of participants from around the world, including researchers and stakeholders from military and Veteran communities. Current performance indicators in the CIMVHR PIP, however, do not reflect the number of individuals reached through this event. To date, reporting has focused on the number of research events rather than the number of individual audience members reached, which is inconsistent with how other sub-components of the Research and Innovation Program report their reach. There is an opportunity for the PIP to be changed to measure both the number of events and the number of individuals reached to better reflect its impact.
The Journal of Military, Veteran and Family Health (JMVFH) continues to see growth in downloads year over year. This growth can be attributed in part to an increase in the number of journal issues (from three to five annually) and expanding marketing and social platform presence.
Initially there was an indicator established to gauge how research information was used by researchers/informed decision making. When revisiting the methodology, it was determined that this indicator would be challenging to measure. As a result, an alternative indicator of number of annual article downloads from CIMVHR’s journal was adopted.
Measuring “use” may be a subjective measure in this instance, if an article is downloaded, one can presume it was read and therefore an indicator of consideration for use, but not a direct measure of research used. The evaluation finds that the current information tracked does not accurately measure how research information is being used. Additional details on the audiences reached and information distributed could provide more clarity as to the extent of reach and potential impact. CIMVHR is also tracking citations from articles published in their peer reviewed journal, and exploring the use of software to enhance data capture. Given the journal’s role as a key source of peer-reviewed military and Veteran health research, and the fact that other components of the Research and Innovation Program also track citations, integrating citation data into the PIP would strengthen overarching program performance measurement. Citations provide a more robust and objective measure of research use than downloads and would contribute to consistency across the program’s performance metrics.
In the winter of 2025, CIMVHR contracted a third party to conduct a review of the organization. The review included an assessment against strategic goals and provided some recommendations to further enable achievement of the goals. One key focus area identified was continuing to enhance measuring impact of CIMVHR activities, including knowledge translation.
Capacity building
In addition to growing organization and institutional partnerships, CIMVHR contributes to growing research capacity for military, Veteran and family health and well-being through the administration of student scholarships and a student community of practice.
For example, between 2014 and 2023, CIMVHR, in partnership with the Royal Canadian Legion, awarded ten scholarships valued at over $300,000. CIMVHR reports that of those who completed their research projects, all have continued scholarly research related to military, Veterans and their families in their careers. As reported in the Journal of Military, Veteran and Family Health in 2024, these investments in capacity have led to an additional 36 peer-reviewed studies cited in 170 articles.Footnote 28
4.1.4 Joint Federal Research Funding Program (JFRFP) Performance
Measuring JFRFP program performance is difficult given the program is early in its lifecycle. As mentioned previously, a performance information profile has not been developed for the program and no performance goals have been established. Only two rounds of funding have been issued (one in 2023–24 and another in 2024–25) supporting a total of 27 research projects. As Table 10 shows, the majority of projects funded were supported by CFHS or DRDC.
| Organization | Number of Projects | Number Completed |
|---|---|---|
| CFHS | 8 | 0 |
| DRDC | 12 | 2 |
| VAC | 7 | 1 |
Source: Veterans Affairs Canada website accessed November 7, 2025.
Of the three research projects completed, only one of those was funded by VAC. Interviews do indicate, however, that the completed project has benefited the department and has been used to inform ongoing policy work.
VAC works in consultation with the partner departments to plan and develop funding opportunities. To date this process has not been driven by a formal process like the other Research and Innovation Program components. The development of guidance documents is further discussed in section 4.4.4.
In terms of reach, funding opportunities are posted on the VAC website and promoted through CIMVHR’s academic network. The department is not currently reporting data related to reach. However, there is an opportunity to track uptake through measures such as web views, CIMVHR email list reach, funding opportunity responses, etc.
4.1.5 Ultimate Outcome
Results for ultimate outcomes are reported at the departmental level through the Departmental Results Framework.Footnote 29 While VAC has multiple ultimate outcomes, the program components of the Research and Innovation Program are linked to a single departmental ultimate outcome – that Veterans are physically and mentally well. As of 2022, this outcome is measured through the Canadian Veteran Health Survey that captures information on the entire population of Veterans, both clients and non-clients. This survey is conducted every two years. Prior to using this survey, the department used the Life After Service Survey (last conducted in 2019) as a means to measure the ultimate outcome. Table 11 highlights results captured as of September 2025.
| Performance Indicator | Target | 2019-20 | 2020-21 | 2021-22 | 2022-23 | 2023-24 | 2024-25 |
|---|---|---|---|---|---|---|---|
| Percentage of Veterans who report that their health is very good or excellent | 50% | -- | -- | -- | 40% | -- | 41% |
| Percentage of Veterans who report that their mental health is very good or excellent | 60% | -- | -- | -- | 49% | -- | 49% |
Source: Canadian Veteran Health Survey
There are no mechanisms in place to measure contributions the components of the Research and Innovation Program might have towards the ultimate outcome. In addition, the target audiences of the funded programs or services are not necessarily Veterans (e.g., family members, service providers, clinicians and researchers). It is hard to attribute impact from the Research and Innovation Program to the ultimate outcome.
4.2 Knowledge Mobilization
Knowledge mobilization emerged as a central theme throughout the evaluation. While definitions vary, it is broadly understood as the process of moving research findings into action to generate real-world impact. Related terms such as knowledge translation, knowledge transfer, and knowledge exchange are sometimes used interchangeably.Footnote 30
There has been an increasing focus and realization that research can be conducted and published for academics, but there is a need to share information in various formats to multiple audiences. Interviews with researchers and VAC staff indicates that while each subcomponent of the Research and Innovation Program does undertake some form or knowledge mobilization, there does not appear to be a central source for Canadian research on Veteran health.
4.2.1 CPCoE Knowledge Mobilization
The CPCoE recognizes knowledge mobilization as an organizational priority and supports it with dedicated personnel and resources. As outlined previously in Tables 4 and 5, the CPCoE tracks and reports each year on its efforts to share research findings and assess their impact. Over the past three years, results indicate that the Centre’s approach to knowledge mobilization has evolved as it becomes more established within the Veteran research community. Appendix E – CPCoE Knowledge Mobilization highlights ongoing and evolving efforts to ensure research reaches those who can benefit from it.
Within VAC, it is too early to report on major changes to policy or legislation as a result of the CPCoE’s work. Interviews do indicate, however, that efforts are being made to expose VAC staff to the Centre’s chronic pain research. For example, VAC staff have participated in CPCoE led events and summits. In addition, quarterly meetings are being held between VAC and the CPCoE where research findings are discussed and are then brought back to the department. VAC staff also attend CPCoE virtual training and on-line events.
CPCoE’s support for the McMaster Health Forum’s Evidence Support Mechanism has contributed to knowledge mobilization within VAC. This initiative, launched in 2022, is a collaborative effort involving the CPCoE, VAC, the Atlas Institute, CFHS, and the Director General Military Personnel Research and Analysis.Footnote 31
Hosted through McMaster University, the McMaster Health Forum aims to synthesize and mobilize evidence to inform health and social policy. It brings together researchers, policymakers, and individuals with lived experience to address complex challenges through evidence-informed decision-making. Through CPCoE funding, VAC has gained access to the Forum’s rapid evidence synthesis program which reviews Canadian and international research. Syntheses produced by the Forum have supported VAC in addressing health questions related to:
- treatment approaches for substance use disorders;
- the use of cannabis for medical purposes;
- health issues affecting women Veterans;
- the link between hearing loss and dementia; and
- the relationship between occupational stress and heart disease.
Interviews with VAC staff suggest that these rapid evidence briefs have been particularly useful in informing updates to VAC’s Table of Disabilities, helping ensure that disability assessments reflect the latest research and best practices.Footnote 32
4.2.2 Atlas Institute Knowledge Mobilization
The Atlas Institute’s approach is based on two principles: engagement and co-creation, with the aim to provide relevant information to those who need it. As highlighted earlier, one of the Atlas Institute’s goals is to increase awareness and understanding, ensuring information gets into the hands of people who need it in an easy to use and understandable format.
The organization has a dedicated knowledge mobilization team and knowledge mobilization is an embedded component of all research. Knowledge products range from resources and tools specific to a topic/population, to plain-language outputs of published research findings. The Atlas Institute’s co-creation model engages Veterans and families in all project aspects, from project design to execution and public launch. The current performance measurements captured by VAC touch on knowledge mobilization (uptake of evidence-based information products and tools, number of knowledge products disseminated, number of audiences reached and satisfaction with the quality of the evidence-based information and tools). In each instance the Atlas Institute has met or exceeded their annual target, and/or is projected to achieve the target by the established date. There may be opportunities to enhance the qualitative measurement in the future (e.g. stakeholder satisfaction, enhancements to processes and research products, etc.).
VAC staff had mixed feedback on the dissemination and awareness of research products from the Atlas Institute. While knowledge mobilization to VAC is not their primary role, there is an opportunity to enhance awareness and knowledge mobilization within the Department to potentially support program management and delivery and policy development. As noted, the Atlas Institute is also a collaborative partner in the McMaster Health Forum’s Evidence Support Mechanism.
4.2.3 CIMVHR Knowledge Mobilization
Two of CIMVHR’s primary outputs, their journal and the annual Forum, serve as key mechanisms to mobilize research knowledge. The journal is open access, allowing unrestricted no-cost access to articles. The Forum brings together researchers and stakeholders, including military members and Veterans, providing an opportunity for a variety of mechanisms to exchange knowledge (e.g. presentations, posters, and networking). Both the journal and the Forum are well established with a wide-reaching international presence.
As an organization focused on academic published research, CIMVHR has identified an effort on improving knowledge translation .Knowledge translation and knowledge exchange are identified as key business activities to help augment the reach and impact of research. Strategic goals outlined annually, along with interviews with CIMVHR staff, demonstrate that CIMVHR is working to try to bridge the gap between academic published research and practical application to stakeholders and audiences outside academia. CIMVHR is exploring ways to measure impact of all its efforts including use of existing data.
4.2.4 JFRFP Knowledge Mobilization
To date, only one research project has been completed for VAC under the JFRFP. While the report is available online through the Perley Health Community of Care website, there is no link to the research on VAC’s website (VAC does provide a short summary online) or on any other Government of Canada website.Footnote 33 The report has contributed to ongoing policy work at VAC, but it has not been widely circulated throughout the department (though the research was presented by the project lead to the VAC-DND Research Collaboration working group). Conversely, research completed through the JFRFP sponsored by DRDC is published on the DRDC website in a searchable database. The database houses more than sixty years’ worth of scientific and technical research produced by or for DRDC.
4.2.5 Knowledge mobilization within VAC
VAC’s Research Directorate conducted an assessment of knowledge transfer and developed a plan in 2019 to improve the dissemination of its own in-house research. This plan was updated in 2022–23 to focus on strategies that ensure VAC-generated research is effectively shared, understood, and applied across the Department. However, the scope of this plan is limited to internal research and does not include mechanisms for integrating external research findings into departmental decision-making or operations.
Currently, VAC does not have a formal structure or designated responsibility for mobilizing research produced by external partners such as the Atlas Institute, the CPCoE, or CIMVHR. While interviews suggest that knowledge is being shared informally, the absence of a formal knowledge mobilization plan limits consistency and clarity on when and how research should inform policy and program decisions. Additionally, there is no known searchable central repository for Canadian research on Veteran health, similar to the database of military research maintained by DRDC or CIHR-funded research databases. Although the CIMVHR Journal serves as a key source of peer-reviewed military and Veteran health research, accessibility to other research remains fragmented.
Recent developments also underscore the importance of addressing knowledge mobilization gaps. A 2025 parliamentary report on the Federal Framework on PTSD identified the creation of a single Canadian repository of guidance information for healthcare providers as a priority. A supporting review conducted by McMaster University’s Trauma and Recovery Lab included a scan of available evidence and guidelines on mental health interventions. McMaster has committed to implementing a knowledge mobilization plan to make this information accessible to Canadians, including military members, Veterans, and service providers. The evaluation notes that VAC may have opportunities to learn from and leverage this approach to strengthen its own knowledge mobilization efforts.
4.3 Lived experience
Lived experience
Lived experience refers to the knowledge and perspective gained through personally encountering and navigating a specific situation or event. It emphasizes direct involvement and first-hand participation, distinguishing it from information derived through research, theory, or second-hand accounts.
Embedding lived experience into research projects takes time and effort. Feedback from both the CPCoE and the Atlas Institute indicate that while projects make take longer, the quality of research is enhanced. And, while it is too early to assess, there may be a positive unintended impact from including individuals with lived experience directly in research planning and conduct - mainly the opportunity to emerge not only as best practice in research, but also providing individuals a voice and a sense of community or purpose that they may not have had otherwise.
The willingness on the part of the Veteran community to offer their lived experience was evident in a recent call for Veteran family members to participate in an Atlas Institute study. More than 200 applications were received within two to three days for a study that only required 30 participants.
The Atlas Institute’s conceptual framework was created to provide the key vision for a system of services and supports reflecting what was being heard from Veterans and their families. As a foundation for engagement, the Atlas Institute sought to co-develop a Veteran and Family engagement framework. They have a Veteran advisory committee, a lived experience Veteran team and a cadre of Veterans and their families who provide various degrees of input and participation. Since its inception in 2022 the group has advised on 65 projects.
"I realized that there was something in all of this that was useful for others, instead of just for myself... I can shift back and forth and see how this fits into the bigger picture."
Veteran participant in digital storytelling workshop
Like the Atlas Institute, the CPCoE has also embraced the lived experience of Veterans as an important component in priority setting, research planning, and research projects.
4.4 Economy and efficiency
As mentioned throughout the report, the program components were initiated at various times between 2019 and 2022. Table 12 highlights annual program expenditures for each of the Research and Innovation Program sub-components evaluated.Footnote 34
| Fiscal year | Atlas (PTSD CoE) | Chronic Pain CoE | CIMVHR | JFRFPFootnote 35 | TOTAL |
|---|---|---|---|---|---|
| 2019-2020 | $1,290,647 | $500,000 | 0 | 0 | $1,790,647 |
| 2020-2021 | $6,265,285 | $4,148,386 | $1,957,713 | 0 | $12,371,384 |
| 2021-2022 | $8,918,164 | $4,306,984 | $2,500,000 | 0 | $15,725,148 |
| 2022-2023 | $9,008,161 | $4,528,497 | $2,500,000 | $200,000 | $16,236,658 |
| 2023-2024 | $9,191,941 | $4,641,355 | $2,500,000 | $2,150,000 | $18,483,296 |
| 2024-2025 | $9,134,525 | $4,641,355 | $2,500,000 | $4,290,714 | $20,566,594 |
| Sub-total | $43,808,723 | $22,766,577 | $11,957,713 | $6,640,714 | $85,173,727 |
Source: VAC Finance
A total of $85 Million was spent on research related program expenditures between 2019-20 and 2024-25. A review of operational data shows that funds allocated were exhausted year over year, with the exception of 2021-22, where 10% of funding lapsed.
Expenditures for the total program components account for less than half a percent of total VAC program expenditures.
Administrative costs
The Department has allocated between five and seven full-time equivalent employees to the Research and Innovation Program between 2020-21 and 2024-25. Administrative costs for sub-programs are not currently tracked by the department as distinct expenditures. As a result of this costing approach, the evaluation team faced limitations in assessing the specific administrative costs associated with delivering individual program components.
Because each sub-component operates under its own contribution agreement or memorandum of understanding, the evaluation team was able to access budget and expenditure data. However, the evaluation did not specifically examine the operational and administrative costs of the arm’s-length organizations. Details on program expenditures and the scale of each organization’s operations in delivering the respective program components are provided in the following sub-sections of the report.
4.4.1 Chronic Pain Centre of Excellence efficiency and economy
As per the terms of the 2023-28 contribution agreement between VAC and the CPCoE, VAC will contribute up to $23,308,395 to the CPCoE over five years with an annual allocation of $4,661,679. The funding is intended to cover up to 100% of the organization’s eligible expenditures, including salaries, travel, materials, audits, communications, rent, capital expenditures, etc.
CPCoE funding from other sources
Under the current funding agreement, any funds collected from external sources by the CPCoE for Veteran chronic pain research result in a dollar-for-dollar reduction in VAC’s contribution. While the CPCoE holds charitable status, this arrangement effectively eliminates any financial advantage to pursuing additional fundraising efforts, as external contributions do not increase the overall funding available for research. Consequently, the CPCoE remains fully reliant on VAC as its sole source of operational and research funding.
This dependency creates several implications or risks for the CPCoE:
- limits financial flexibility – the CPCoE cannot leverage philanthropic or private-sector contributions to expand research capacity or invest in innovative projects beyond the CPCoE’s current scope;
- reduces incentive for partnerships – potential collaborations with industry, foundations, or donors may be discouraged, as their contributions would not result in net new resources for the organization;
- strategic risk – full reliance on a single funding source exposes the CPCoE to financial vulnerability should VAC’s budget priorities shift or funding levels decrease in the future.
From a VAC perspective, however, limiting funding opportunities mitigates the risk of work falling outside the scope of the department, its mandate, and the direction set out in the original mandate letter to the minister.
If/when any contribution agreement amendments are being considered, these points should be taken into consideration.
Reporting requirements
The contribution agreement also outlines CPCoE reporting requirements which include:
- quarterly progress reports;
- annual financial statements;
- annual performance and GBA Plus reports;
- asset inventories;
- audit reports; and
- final reconciliation and claims.
Interviews indicate that CPCoE financial reporting has been timely and no major concerns have been identified. The evaluation did, however, identify an area of risk with regard to the “just in time” nature of VAC funding installments. The CPCoE does not have the ability to carry forward funds from one fiscal year to the next and relies on the arrival of VAC funding during the first week of April to cover expenses. If the funding does not arrive on time as has happened in the past, the CPCoE has few options to mitigate as they cannot receive funding from other sources nor can they establish a line of credit.
Administrative expenses
The current VAC expenditure reporting template uses pre-determined categories aligned with eligible expenditures outlined in the contribution arrangement (e.g., salaries and benefits, rent, utilities). Due to the nature of the centre’s work (research, training, and knowledge mobilization) activities rely heavily on individual effort (primarily salaries). However, submitted salary expenditure do not distinguish between administrative and project-related work, making it difficult to measure direct versus indirect costs. Excluding salaries and benefits, CPCoE’s operational and administrative expenses have remained consistent at approximately 12% to 15%.
There is no expectation of a return on investment directly to the department from the research sponsored by the CPCoE, which is reflected in the performance indicators that measure reach rather than impact. An evaluation of value for money for VAC is not possible at this time, partly due to the hands-off nature of the relationship between VAC and the CPCoE (as prescribed in the contribution agreement) and partly due to the relative “newness” of the centre and the research it is producing (i.e., it takes time for a body of research to be conducted, validated, and translated into action). Interviews suggest that research sponsored by the CPCoE has not yet resulted in policy change at VAC, however it has been taken into consideration when reviewing areas such as treatment benefits and the Table of Disabilities. While it may not yet be possible to quantify a financial return for the department, there is intrinsic value in that the CPCoE is advancing the body of research around Veteran chronic pain and building capacity within the research community. This, in turn, has potential to shape future decisions by VAC and future treatments for Veterans.
4.4.2 CIMVHR Efficiency and economy
Previously, CIMVHR operated under a contribution agreement with Health Canada.
In 2020, VAC signed a ten-year contribution agreement to support CIMVHR. Under this arrangement, CIMVHR is considered a funded “project” under the project authority, Queen’s University. As part of the arrangement Queens provides services to CIMVHR, for a fee, including human resources, legal support, accounting, and access to staff pension plans. Interviews indicate that the administrative arrangement with Queens offers value for money.
Under the terms of the contribution agreement, VAC provides $2.5 million annually towards CIMVHR’s operations, however, the Department remains “at arms length” and has no say in the organization’s day-to-day activities. VAC funding can be used for eligible operating expenses including salaries and benefits, travel and accommodations, materials and supplies, performance measurement, rent and utilities, hospitality, and communications. Approximately 60% of CIMVHR’s overall expenditures relate to salary and benefits. Other funded activities include preparing and hosting the annual Forum, seeking submissions and editing the journal, preparing knowledge products, hosting workshops and sessions, etc. Interviews indicate VAC’s stable funding has allowed CIMVHR to continue operations that would not be possible otherwise.
Funding from other sources
VAC funds core operations, in addition to this funding CIMVHR continues to partner with and seek funding from other sources (e.g., True Patriot Love Foundation, The Royal Canadian Legion, and War Amps Canada) to fund various activities such as research and scholarships. As per the agreement between VAC and CIMVHR, the organization is required to disclose the total contribution from all sources in support of the project as well as total expenditures.
Administrative costs
CIMVHR must manage its activities and spending within the limits of the annual contribution, which does not increase with inflation. As the funding agreement continues over time, the fixed annual contribution loses value as costs and wages go up. To maintain consistent outputs and outcomes, it may be worth considering the inclusion of a Consumer Price Index (CPI) adjustment in the next contribution agreement.
VAC’s annual contribution supports CIMVHR’s day to day operations. The evaluation finds that stable funding ensures core CIMVHR products and activities (like the journal, Forum, and partnerships) can continue to support growth and capacity building in the Veteran health research field.
Reporting requirements
The funding agreement requires both quarterly and annual reporting, which VAC has received to date. These reports include budgets and actual expenditures for each period. According to interviews and a review of departmental documents, initial reporting issues have been resolved and the reporting format was updated in 2023-2024.
4.4.3 Atlas Institute economy and efficiency
As per the terms of the 2022-27 contribution agreement between VAC and the Atlas Institute (the CoE of PTSD and related mental health conditions), VAC will contribute up to $46,000,000 over five years with an annual allocation of $9,200,000. Terms include covering 100% of eligible expenditures, including salaries and benefits, travel, materials and supplies, communication, rent and utilities, equipment, etc. Like the CPCoE and CIMVHR, there is no annual inflation factor built into the contribution agreement.
Reporting requirements
The funding agreement requires quarterly and annual reporting. These reports have been received to date. Reporting includes quarterly and annual budgets and actual expenditures. VAC staff interviewed reported no issues or concerns with reports received. Similar to the CPCoE, current financial reporting from the Atlas Institute is focussed on eligible expenditure categories and does not enable the evaluation team to distinguish between direct and indirect research costs.
Funding from other sources
Similar to the CPCoE, the Atlas Institute is fully funded by VAC. It is the responsibility of the Atlas Institute to inform VAC of any financial assistance received from other sources, as well as the total expenditures made in relation to the Project. If funding exceeds 100% of project costs/eligible expenditures, Canada may recover funds. The risks identified relating to the CPCoE in section 4.4.1 are also considered relevant for the Atlas Institute.
Administrative costs
The Atlas Institute is larger than the CPCoE, consisting of over 50 staff in a range of disciplines (applied and clinical research, partnerships, stakeholder engagement, knowledge mobilization and implementation, strategic operations, communications and strategic advisors).The bulk of the institute’s expenditures are operational, most of which is attributable to salaries and benefits.
The evaluation currently lacks sufficient evidence to conclusively determine value for money, primarily because the impact of research is inherently difficult to measure. However, there are indicators of foundational value. The Atlas Institute has demonstrated ongoing growth through the expansion of its partnership network, increased engagement within its stakeholder reference group, and a rising output of research papers, training sessions, and other knowledge mobilization products. (These findings are supported by document review, available data and qualitative feedback from interviews).
It is important to note that evaluating the value of research in a broad health and well-being context—particularly when not directly linked to departmental programs and services—tends to be more subjective in nature (e.g. may not necessarily result in changes in policy or treatments).
4.4.4 Joint Federal Research Funding Program efficiency and economy
VAC, DND, and CAF work together to fund and manage research projects through the Joint Federal Research Funding Program. DND and CAF provide money to VAC not only to support the research itself but also to cover the costs VAC incurs in organizing and overseeing these projects. VAC handles its own projects within its existing budget, which helps keep additional administrative costs low. Defense Research and Development Canada (DRDC) serves as the science and technology organization within DND and is the principal signatory of the JFRFP MOU on behalf of DND. The Canadian Forces Health Services Group (CFHS) fulfills all military health system functions for the CAF (including research) and holds responsibility for the JFRFP within the CAF.
The JFRFP can distribute two types of funding depending on the level of risk involved:
- grants which are used for low-risk projects that require less oversight; and
- contributions which can be used for higher-risk projects which can include more reporting and auditing.
This approach can help match the level of administrative effort to the risk of each project, however, to date, no contributions have been awarded.
According to the MOU, each participating department must commit at least $500,000 per year to fund research projects (though VAC has recently dropped its contribution to $350,000Footnote 36). Commitments for fiscal years 2023-24 and 2024-25 are shown in Table 13.
| Organization | 2023-24 (actual) | 2024-25 (actual) |
|---|---|---|
| DRDC | $1,000,000 | $1,500,000 |
| CFHS | $500,000 | $2,444,390 |
| VAC | $350,000 | $350,000 |
| Total | $1,850,000 | $4,294,390 |
Source: VAC Finance Division
Funding agreements for research can span multiple years. VAC has the flexibility to tie payments to specific milestones if necessary to help ensure that projects stay on track and that funds are used responsibly.
For projects sponsored by DND and the CAF, VAC charges a fixed administrative fee of $50,000 per year plus 4.25% of each individual total project’s total valueFootnote 37. This fee structure allows VAC to partially recover project management costs. As Table 14 indicates, VAC currently allocates approximately $200,000 in salary for administration of the JFRFP.
| Classification | Position | Classification | Time dedicated to JFRFP | Net Forecast |
|---|---|---|---|---|
| WP-6 | Indeterminate FT | WP-6 | 13.6% | $18,488 |
| EC-1 | Determinate FT | EC-1 | 100% | $65,131 |
| AS-6 | Indeterminate FT | AS-6 | 100% | $115,695 |
| Total | $199,314 |
Source: VAC Finance Division
Further analysis indicates that total salary spent is actually in the range of $231,000
when taking into consideration effort as well as unfunded labour being paid for by other areas of the department. Additional administration costs of approximately $22,000 are also incurred annually for translation, communications, and other miscellaneous expenses. Both the administrative effort required to manage the program and feedback from VAC interviews suggest that the original fee structure did not fully account for the actual workload involved. During the reporting phase of the evaluation, the partner organizations agreed to amend the MOU to change the per project administrative fee model from 3% to 4.25% to more accurately reflect the administrative costs associated with delivering the program.
An analysis of funds transferred from the partner organizations in 2024-25 compared to the estimated administrative costs to deliver the program indicates that the new fee structure is more in line with actual costs. However, at the time of the evaluation there were two unfunded positions working in the JFRFP unit; if these positions remain unfunded/not permanent there is a risk of insufficient human resources to support the delivery of the program.
As can be seen in Appendix F, there were 27 projects funded through the JFRFP between 2023-24 and 2024-25. Individual project values can range depending on project topic and scope. With only two years of data there is insufficient evidence to support trend analysis.
The program includes several financial controls to ensure money is used appropriately. Projects must report any other sources of funding to avoid being overfunded and VAC has the ability to tie payments to performance milestones if necessary. Oversight is adjusted based on the risk level of each project, which helps control costs while still ensuring accountability.
Interviews with stakeholders noted that it can be challenging to effectively plan funding transfers well in advance which may result in delays in project approvals. It was emphasized that the program is meant to support research, not act as a contracting service. Interviewees generally agreed that the JFRFP is flexible and collaborative. While it is too early to fully assess efficiency, there are indications that the process is more timely compared to previous models (e.g., contracts).
Regular meetings with partner departments have been occurring since 2024. The evaluation team notes a few changes have occurred throughout the conduct of the evaluation including amendments to the MOU administration cost calculations and working towards enhanced supporting guidance documentation (e.g., the creation of a roles and responsibilities document, assessment committee terms of reference, templates, etc.). It is too early to comment on the impact of these changes, however it is reasonable to assume they will help improve cost-effective delivery of the program and enhance the rigour and efficiency of funding opportunity development and assessment process.
4.4.5 Research collaboration
Departmental planning documents outline an expectation that the program components work together effectively to ensure research efforts are coordinated and duplication is minimized. The Atlas Institute, CIMVHR, and the CPCoE have established a statement of agreement committing the groups to meet twice annually. These meetings aim to align their respective efforts, minimize duplication, and identify efficiencies and opportunities for collaboration. The overarching goal is to foster a coordinated and collaborative research environment.
Program design documents highlight that the department will support coordination of activities between CIMVHR, the CoE on Chronic Pain, the existing CoE in PTSD and Related Mental Health Conditions, and Veteran and Family Well-being Fund initiatives. Interviews indicate ongoing dialogue between VAC, the centres of excellence, and CIMVHR regarding priority setting and the avoidance of overlapping work. Maintaining continuous communication among these organizations is essential to ensure their activities remain complementary and strategically aligned.
5.0 Summary of findings
The evaluation confirms a sustained need and demand for research, collaboration, and knowledge dissemination related to the health and well-being of military members, Veterans, and their families. The Research and Innovation Program’s intent is consistent with Government of Canada priorities and departmental roles and responsibilities.
The priorities of the program sub-components align with the objectives of the Research and Innovation Program and are informed by input from Veterans and their families. While the program demonstrates strong alignment with its objectives, there are opportunities to strengthen its performance measurement framework. Current indicators are inconsistent across sub-components and mechanisms to measure contributions toward ultimate outcomes are absent. And, while the Atlas Institute, the CPCOE, and CIMVHR have established meaningful activities and networks, refinements to performance indicators, methodologies, and reporting systems are needed to capture success. The JFRFP lacks performance indicators entirely and related measures are not captured in departmental reporting.
Knowledge mobilization was a recurring theme in discussions with staff at VAC, the Atlas Institute, the CPCOE and CIMVHR. While knowledge mobilization is emphasized across all program sub-components, the absence of a centralized, searchable repository for Canadian research on Veteran health poses limitations. Additionally, there is no formal mechanism to ensure research findings flow back to VAC. While regular communication occurs among sub-components (and VAC) to avoid duplication and to align research priorities, further coordination would enhance efficiency as the organizations mature.
Financially, program funds are being spent with minimal lapse. CPCoE administrative expenses are consistent with comparable institutions. However, VAC’s role as the sole funder of the centres of excellence presents sustainability risks. The CIMVHR funding model also poses a risk as the fixed annual contribution is increasingly constrained by rising costs. Finally, adjustments to the JFRFP administration fee structure have improved alignment with VAC’s actual costs, though risks remain regarding human resource capacity if key positions are not permanently secured.
5.1 Conclusion and recommendations
The Research and Innovation Program is meeting its core objectives and remains relevant to the needs of Veterans and their families. Its sub-components contribute meaningfully to research capacity and knowledge mobilization in Canada. However, improvements to performance measurement, coordination, and sustainability are required to ensure long-term impact and efficiency. Strengthening indicators, establishing mechanisms for knowledge sharing, and addressing funding and resource risks will position the program to better achieve its intended outcomes and maintain alignment with federal priorities.
The evaluation team, therefore, makes the following recommendations:
Recommendation #1
The Assistant Deputy Minister Strategic Policy, Planning and Performance and the Assistant Deputy Minister of Service Delivery review and update the current Research and Innovation Program Performance Information Profile to:
- develop and implement performance indicators to measure success of the Joint Federal Research Funding Program; and
- enhance conciseness and consistency of performance measures and methodologies across the program sub-components
| Action and Rationale | Expected Completion /Implementation Date | ADM Accountable for Action |
|---|---|---|
| The Director General, Policy and Research Division will work in collaboration with the Director General, Strategic Planning, Results and Cabinet Business to develop and implement performance indicators to measure success of the Joint Federal Research Funding Program. | December 31, 2026 | Assistant Deputy Minister of Strategic Policy, Planning and Performance |
| The Director General, Health Professionals Division; Director General, Policy and Research Division; and Director General, Strategic Planning, Results and Cabinet Business will work in collaboration to propose, where appropriate, opportunities to enhance conciseness and consistency of performance measures and methodologies across the Research and Innovation Program, including sub-components. | June 30, 2027 | Assistant Deputy Minister of Service Delivery and Assistant Deputy Minister of Strategic Policy, Planning and Performance |
Recommendation #2
The Assistant Deputy Minister Strategic Policy, Planning and Performance develop a departmental knowledge mobilization plan, including how externally funded research is funneled back into VAC to support program management and policy development.
| Action and Rationale | Expected Completion /Implementation Date | ADM Accountable for Action |
|---|---|---|
| The Director General, Policy and Research Division will lead development of a plan, in collaboration with OPI’s across the Department, including Communications and Service Delivery, and with our partners in the Research and Innovation Program (i.e., Atlas, CPCoE, and CIMVHR). The work will include developing a research/policy/service delivery continuum model, establishing governance, defining roles and responsibilities, and developing an impact model to demonstrate how externally funded research supports VAC policy development, program management, service delivery, and associated results. | June 30, 2028 | Assistant Deputy Minister of Strategic Policy, Planning and Performance |
Appendices
Appendix A: Sample research projects sponsored by the CPCOE
The CPCoE has disbursed over $8.6 million in funding between 2020-2025. Table 15 shows a sample of the work sponsored by the CPCoE.
| Research Project Title | Lead Institution | Status |
|---|---|---|
| Interventions to Prevent Chronic Pain after Orthopedic Surgery | McMaster University | Complete |
| Treatment preferences among Canadian military Veterans with chronic low back pain | McMaster University | Complete |
| Developing a Veteran Identifier in Health and Social Data | Queen’s University | Complete |
| Integrating Canadian Veteran needs in identifying effective self-education tools for medical cannabis use in chronic pain | University of Waterloo | Complete |
| Veterans Cannabis Therapy Outcomes Registry | McMaster University | Complete |
| Yoga for Veterans with Chronic Pain | University of British Columbia | Complete |
| Considerations for Ketamine in the Effective Management of Chronic Pain for Veterans | St. Joseph’s Health Care | Complete |
| Intergenerational Transmission of Chronic Pain in Canadian Veterans and their Children | University of Calgary | Complete |
| The Chronic Pain Experiences of Military Personnel, Recently Retired or Discharged Veterans, and Healthcare Providers: A Systematic Review and Qualitative Meta-Synthesis | The Methodologists Corp. | Complete |
| Examining Similarities and Differences Between Veterans and Civilians Regarding their Chronic Pain and Mental Health Experience | McMaster University | Complete |
| A Feasibility Study on the Ability to Scale an Interdisciplinary Pain Management Program for Canadian Veterans across Canadian Provinces | Lifemark Health Group | Complete |
| Understanding Sex and Gender Differences in the Experience of chronic Pain and its Management | Western University | Complete |
| Testing the feasibility, tolerability and potential efficacy of ketamine assisted psychotherapy for treating comorbid chronic pain posttraumatic stress disorder in Veterans of the Canadian Armed Forces | Queens University | Ongoing |
Source: veteranschronicpain.ca accessed August 15, 2025
Appendix B: Sample research projects sponsored by the Atlas Institute
Table 16 shows a sample of the work sponsored by the Atlas Institute.
| Research project | Lead Institution | Status |
|---|---|---|
| Clinical trial showing neurofeedback training can help reset brainwaves and help with emotional regulation in people with PTSD | Atlas Institute | Complete |
| Identity in turmoil: Investigating the morally injurious dimensions of minority stress | Atlas Institute | Complete |
| A tale of two targets: Examining the differential effects of posterior cingulate cortex- and amygdala-targeted fMRI-neurofeedback in a PTSD pilot study | Atlas Institute | Complete |
| Improving machine-learning-driven development and identification of PTSD phenotypes | McMaster University | Complete |
| Informing responses to intimate partner violence in military or Veteran populations within Canada | Phoenix Australia Centre for Posttraumatic Health | Complete |
| Moral injury outcome scale (MIOS) | Boston University | Complete |
| Understanding how adjustment to civilian life relates to the mental and behavioural health of Canadian Armed Forces Veterans | Atlas Institute | Ongoing |
| Treatment-resistant PTSD | The MacDonald Franklin OSI Research Centre | Ongoing |
| Psychological, autonomic, and sleep (PAS) profiles in post-traumatic stress disorder and depression | University of Ottawa | Ongoing |
| Veterans’ Mental Health and Media Analysis Study | McGill University | Ongoing |
| Qualitative Interviews with Healthcare Workers Surrounding Their Experience of COVID-19 Related Moral Injury | McMaster University | Ongoing |
| Study showing that people with PTSD experienced reduced reliving and distress symptoms as a result of fMRI-based neurofeedback targeting an area of the brain associated with emotion, thinking about oneself and memory | Atlas Institute | Complete |
| The role of peer support in responding to moral injury in public safety personnel | Atlas Institute | Complete |
| Brain Measures Linked to Hyperarousal in PTSD using MRI Imaging | University of Ottawa | Ongoing |
| Women Veteran's Health Survey | Atlas Institute | Ongoing |
Source: https://atlasveterans.ca/our-approach/research/ accessed October 10, 2025
Appendix C: Sample research projects sponsored by CIMVHR
CIMVHR has sponsored over 100 projects in the past 12 years through funding provided by various donors. It should be noted that VAC’s current contribution to CIMVHR is used for administrative purposes and is not used to directly fund research.
| Research project | Lead Institution(s) |
|---|---|
| Uncovering Barriers and Facilitators of Competitor and Caregiver Experience in a Winter Context: An Invictus Games Research Legacy Project | Western University and Lawson Health Research Institute |
| An advanced virtual training system for multi-articulating prosthesis control | University of Alberta |
| one-anchored prostheses and the military: A review of literature and evaluation of their compatibility with military service in the Canadian Armed Forces | University of Alberta; University of Montreal |
| Collaborative paths to understanding: Mental health and wellbeing impacts of participation in the IG2025 | McMaster University |
| Advancing research on servicewomen and women Veterans of the Canadian Armed Forces | Mount Saint Vincent University |
| Sharing of Military Veterans' Mental Health Data Across Canada: A Scoping Review | Dalhousie University, Nova Scotia Health Authority-Operational Stress Injury Clinic |
| Literature review on "Challenges faced by military and public safety and security personnel supporting disaster relief operations" (Task 63) | Lawson Health Research Institute |
| Assessing the needs of Canadian Veterans with amputations and the individuals who care for them | Western University and Lawson Health Research Institute |
| Analysis of data of a lab study on alternative torso-borne armour and load carriage equipment on female varsity-level athletes | University of Guelph |
| Literature Review: Military and Veteran Volunteerism in Canada | Queens University |
| Environmental Scan: Military Creative Arts Initiative | University of British Columbia |
| Literature review on vision requirements for emerging display technologies in military aviation | York University |
Source: https://cimvhr.ca/funded-research-projects/ accessed November 18, 2025.
Appendix D: Gender based analysis plus (GBA+) activity examples
| Organization | Details |
|---|---|
| Atlas Institute | The Atlas Institute recognizes and reflects diverse perspectives by:
|
| CPCoE |
|
| CIMVHR |
|
| JFRFP |
|
Appendix E: CPCoE knowledge mobilization
| Engagement Tool | 2022–23 | 2023–24 | 2024–25 |
|---|---|---|---|
| Bilingual Website Maintained | 1 | 1 | 1 |
| Mailing List | 15,474 | 14,555 | 16,935 |
| Podcast Episodes Produced | 20 | 17 | 28 |
| Podcast Listeners | -- | 2,753 | 3,642 |
| Publications | 1 | 10 | 7 |
| Quarterly Newsletter | 4 | 4 | 4 |
| Social Media Accounts Maintained | 4 | 4 | 4 |
| Website Visits | 14,464 | 19,173 | 53,190 |
| Annual Workshop Audience | 93 | 105 | 112 |
| Educational Guide/Toolkit | -- | 2 | 2 |
| Educational Video | -- | 1 | 1 |
| Infographics | -- | 17 | 3 |
| Plain Language Summaries | -- | 4 | 4 |
| Reports | -- | -- | 2 |
| VAC Stakeholder Conference/Women’s Forum Audience | -- | -- | 200 |
| 2SLGBTQI+ Veterans Forum | -- | -- | 100 |
| CIMVHR Forum | -- | -- | 750 |
| Google Search Impressions | -- | -- | 106,902 |
| Invictus Games Audience | -- | -- | 400 |
| Pain Talks – Montreal Audience | -- | -- | 200 |
| Patient-Centered Outcomes Research Institute | -- | -- | 200 |
| Promotional video | -- | -- | 1 |
| Royal Canadian Legion 49th Dominion Convention | -- | -- | 1,000 |
| Social Media Account Followers | -- | -- | 4,653 |
| Quebec Provincial Pain Symposium Presentation | -- | 200 | -- |
| Canadian Pain Society Scientific Meeting Presentation | -- | 350 | -- |
| Rapid Response Synthesis | -- | 4 | -- |
| September 2023- CPCoE Stakeholders Conference | -- | 120 | -- |
| Blog posts | 3 | -- | -- |
| Dialogue Summary from Round Table | 1 | -- | -- |
| Educational Webinars (2 total, 1Hr each) Audience | 1,848 | -- | -- |
| Evidence Brief from Round Table | 1 | -- | -- |
Source: AED analysis of CPCoE quarterly reports located on VAC’s POIS system
Appendix F: Projects funded through JFRFP (2023-24 through 2024-25)
As of March 31, 2025, there were 27 research projects funded through the JFRFP. As Table 20 shows, VAC has supported 7 projects through the program over the two years.
| Research Project Title | Lead Institution | Funding Source | Status |
|---|---|---|---|
| Development of new approaches to improve the supply of universal “O‑type” red blood cells | University of British Columbia | CFHS | Ongoing |
| Canadian Armed Forces Health Survey (CAFHS 2019) data analysis to examine health trends and factors affecting Canadian Armed Forces (CAF) women and gender‑diverse members | McMaster University | CFHS | Ongoing |
| Systematic Review Exploring the Possible Effects of Military Occupational Exposures on Reproductive Health | University of Toronto | CFHS | Ongoing |
| Needs Assessment to identify priority health research areas for women and diverse members in the Canadian Armed Forces, and to identify existing barriers to carrying out health research for these populations | Lawson Research Institute | CFHS | Ongoing |
| Environmental scan and evaluation of key attributes of training scenarios involving moral‑ethical dilemmas for military personnel | Lawson Research Institute | DRDC | Complete |
| Battlefield evacuation optimization during a mass casualty incident | Toronto Metropolitan University | DRDC | Ongoing |
| Human mental states in military personnel to detect bias in human‑autonomy teaming | Institut national de la recherche scientifique | DRDC | Ongoing |
| PET Tau Brain Imaging and Blood‑Based Molecular Biomarkers of Tauopathy | Centre for Addiction and Mental Health | DRDC | Ongoing |
| Feasibility Study On Health Outcomes for Women and Diverse Members in the Canadian Armed Forces | University of New Brunswick | CFHS | Ongoing |
| Experience, access to care and support | Université de Sherbrooke | CFHS | Ongoing |
| Barriers to access and use of contraception in the Canadian Armed Forces (CAF), other military forces, and Canadian and Global populations | Université de Sherbrooke | CFHS | Ongoing |
| AI‑enabled Transfusion Algorithm for Personalized Trauma Care | Sunnybrook Health Sciences Centre | DRDC | Ongoing |
| Review of the experiences and biopsychosocial impacts of the menopause transition (perimenopause, menopause and post‑menopause) on women Veterans | The Governors of University of Alberta | VAC | Ongoing |
| Review of novel, emerging and alternative mental health interventions for women Veterans | Humber River Health | VAC | Ongoing |
| Review of links between Military Occupational Exposures and cancers in women Veterans | Institute for Work and Health | VAC | Ongoing |
| Vision requirements for Extended Reality displays in military aviation | York University | DRDC | Ongoing |
| Measurement‑based care in military and veteran mental health care systems | Ottawa Hospital Research Institute | CFHS | Ongoing |
| Evaluating Trauma‑Informed Support for Military Personnel and Enhancing Access to Resources using AI | Sheridan College | DRDC | Ongoing |
| Environmental Scan: Best Practices and Approaches to models of care for aging populations | Perley Health (The Perley and Rideau Veteran’s Health Centre) | VAC | Complete |
| Biophysical assessment of Canadian Armed Forces clothing with a sweating thermal manikin | University of British Columbia | DRDC | Complete |
| Exploring the biopsychosocial impacts of pelvic health issues for women Veterans | University of Ottawa | VAC | Ongoing |
| Exploring the experiences and impacts of interpersonal violence affecting Veterans and their families | Mount Saint Vincent University | VAC | Ongoing |
| Comprehensive literature review of pelvic floor dysfunction in Canadian Armed Forces women | Université de Sherbrooke | DRDC | Ongoing |
| Development of a functional test battery for concussion/brain injury to promote recovery and reduce future risk of potential brain and musculoskeletal injuries | The Governing Council of the University of Toronto | DRDC | Ongoing |
| Feasibility of IV Ketamine for the treatment of traumatic brain injury and depression | Keenan Research Centre for Biomedical Science at St. Michael’s Hospital | DRDC | Ongoing |
| Operational colour vision requirements for RCAF pilots | University of Waterloo | DRDC | Ongoing |
| Experiences of LGBT purge survivors with Veterans Affairs Canada Programs and Services | Lawson Research Centre | VAC | Ongoing |
Source: Veterans.gc.ca accessed August 21, 2025
Appendix G: Logic models
The following logic models in Figures 3 and 4 were in place during the period the evaluation was conducted.
Figure 3 – Atlas Institute Logic Model
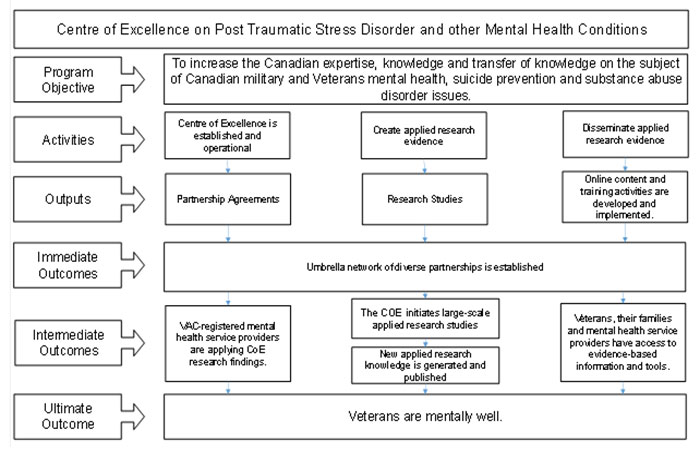
Transcript - Figure 3
The diagram shows the logic model for the Centre of Excellence on Post-Traumatic Stress Disorder and Other Mental Health Conditions (the Atlas Institute). The program objective is to increase Canadian expertise, knowledge, and transfer of knowledge on military and Veteran mental health, suicide prevention, and substance abuse disorder issues.
Activities include establishing and operationalizing the Centre of Excellence, creating applied research evidence, and disseminating that evidence through online content and training activities. These activities produce outputs such as partnership agreements and research studies.
The immediate outcome is the establishment of an umbrella network of diverse partnerships.
Intermediate outcomes follow, where VAC-registered mental health service providers apply Centre of Excellence research findings, the Centre initiates large-scale applied research studies, new applied research knowledge is generated and published, and Veterans, their families, and mental health service providers gain access to evidence-based information and tools.
The ultimate outcome is that Veterans are mentally well.
Source: 2023 CPCoE Priority Setting Report
Figure 4 – Research Funding Program logic model
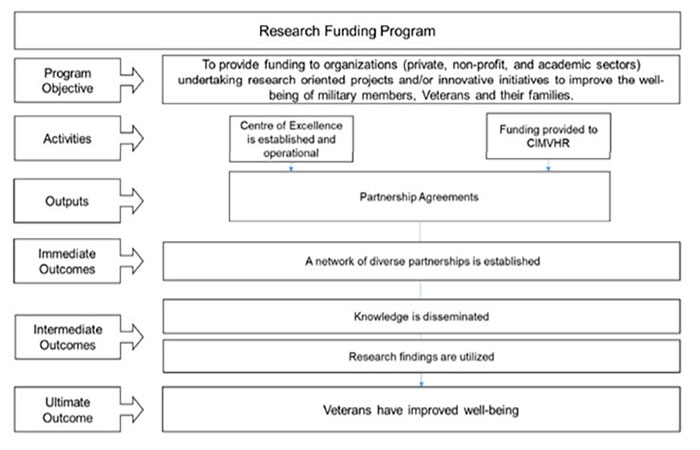
Transcript - Figure 4
The diagram illustrates the structure and logic of the Research Funding Program.
At the top, the program objective is stated: to provide funding to organizations in the private, non-profit, and academic sectors for research-oriented projects and innovative initiatives that improve the well-being of military members, Veterans, and their families.
The next level shows activities, which include establishing and operationalizing a Centre of Excellence and providing funding to CIMVHR. These activities lead to outputs, represented by partnership agreements.
From these outputs, the program achieves immediate outcomes, such as the establishment of a network of diverse partnerships. Over time, this results in intermediate outcomes, where knowledge is disseminated and research findings are utilized. Ultimately, the program aims to achieve its ultimate outcome: improved well-being for Veterans.